WOUNDS AND WOUND CAREAll aspects of skin and soft tissue wounds, including acute surgical wounds, pressure ulcers and all forms of leg ulceration, are encompassed in the specialty of tissue viability. Wound care can be a challenging and complex area of practice, and nurses must take individual responsibility for updating their knowledge, skills and ongoing competence. If in doubt about the care of a wound, seek advice from a more experienced colleague or a tissue viability nurse specialist. Optimum care of a wound requires an understanding of wound healing, microbiology, asepsis, dressings, pain, pharmacology, psychosocial factors and ethics, and use of good communication skills. Diabetic foot wounds need referral to the podiatry team for assessment. Wound healing principlesThe healing process - the restoration of cellular structures and tissue layers – is a complex series of overlapping stages described as:
Broadly, there are two categories of healing:
A non-healing or chronic wound can be defined as one that is failing to progress in a timely fashion through an orderly sequence of repair. Factors that influence healing include:
HSE. National wound management guidelines 2018. https://healthservice.hse.ie/about-us/onmsd/quality-nursing-and-midwifery-care/hse-national-wound-guidelines-2018.html Evidence-based management strategies for treatment of chronic wounds Werdin F, Tennenhaus M, Schaller HE, Rennekampff H. Eplasty 2009; 9: e19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2691645/ Wounds UK. Best Practice Statement: Improving holistic assessment of chronic wounds; 2018 https://www.wounds-uk.com/resources/details/best-practice-statement-improving-holistic-assessment-chronic-wounds Tissue Viability Society https://tvs.org.uk Wound Care Alliance UK https://www.wcauk.org Practice Nurse featured articles The art – and science – of wound healing Sylvie Hampton Healing wounds: where can it go wrong? Elizabeth Merlin-Manton WOUND ASSESSMENTThorough assessment of a wound is the basis for an appropriate dressing selection and management plan. Document:
Scottish Wound Assessment and Action Guide (SWAAG); 2021 https://www.healthcareimprovementscotland.org/our_work/patient_safety/tissue_viability_resources/wound_assessment_action_guide.aspx Healthcare Improvement Scotland. Assessment Chart for Wound Management: December 2020. General wound assessment chart, includes diagrams to document location and template for treatment plan. https://www.healthcareimprovementscotland.org/our_work/patient_safety/tissue_viability_resources/general_wound_assessment_chart.aspx Other tissue viability tools are available at https://www.healthcareimprovementscotland.org/our_work/patient_safety/tissue_viability.aspx The wound bedDifferent types of tissue predominate in the wound bed at different stages of healing. Each needs appropriate management.
ExudateStrikethrough of exudate can increase the risk of bacterial contamination. Prolonged or heavy exudate production may be caused by infection or colonisation, or contamination by a foreign body. If there is associated oedema, limb elevation may be helpful. Colonised woundOrganisms have multiplied to the point that they interfere with healing, but have not invaded surrounding tissue. There is no inflammation, or cellulitis, but the tissue is dull, with dark red granulation tissue that bleeds easily. Wound is malodorous, and healing is delayed. Management aims
Infected woundBacteria have multiplied in the wound and are provoking a host reaction. Clinical signs of infection include:
Signs of systemic infection include:
Management aims
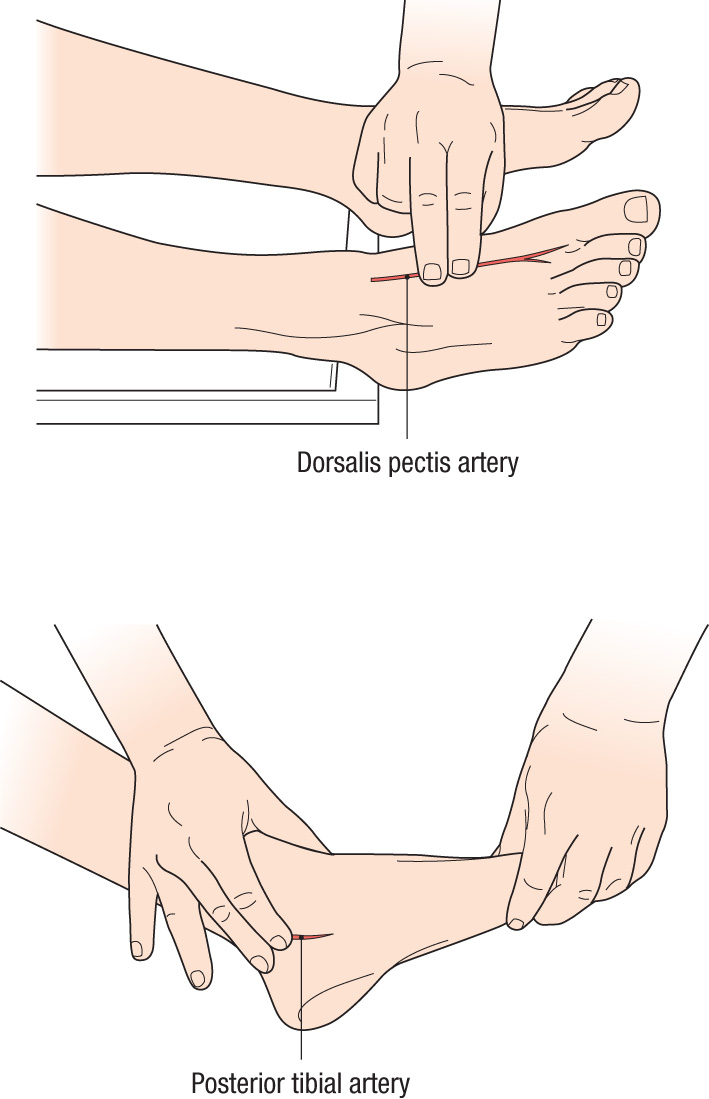
NICE NG152. Leg ulcer infection: antimicrobial prescribing; 2020 https://www.nice.org.uk/guidance/ng152 LEG ULCER ASSESSMENTA leg ulcer - a break in the skin on the lower leg that takes more than 6 weeks to heal - is commonly the result of vascular insufficiency: chronic venous hypertension (a venous ulcer, the most common) or of poor arterial blood supply (an arterial ulcer). Because arterial and venous leg ulcers need different management - compression therapy is dangerous for patients with arterial disease - an important part of leg ulcer assessment is to assess arterial sufficiency by calculating the ankle brachial pressure index (ABPI). ABPI = highest ankle systolic pressure/highest brachial systolic pressure A hand-held Doppler device and a sphygmomanometer and cuff are used to compare ankle and brachial systolic blood pressure. VENOUS ULCERRisk factors
Presentation
Staining (pigmentation) of the skin, induration (hardening, ‘woody’ feel), varicose eczema and oedema.
Management aims
Patient. Venous leg ulcers Professional reference; 2016. https://www.patient.co.uk/doctor/venous-leg-ulcers-pro Diagnosis and management of venous leg ulcers, 2018. BMJ 2018;362:k3115 https://www.bmj.com/content/362/bmj.k3115 ARTERIAL ULCER
Risk factors
Presentation
Management aims
MIXED ULCER (elements of venous and arterial disease)Presentation
Management aims
Before treatment
During treatment
Practice Nurse featured article The art – and science – of wound healing Sylvie Hampton OTHER WOUNDS, INJURIESBites - human and animalHuman bites account for 4-23% of bite injuries, and may be particularly prone to infection (occurring in 9-50% of human bites). Complications include septicaemia, septic arthritis and tenosynovitis, and very rarely, tetanus. Dog bites account for 60-90% of bites, and characteristically involve puncture wounds from the canine teeth, and stretch lacerations. Infection occurs in 2-30% of dog bites. Cat bites account for 5-20% of bite injuries and are also prone to infection. Management of any bite involves removal of any foreign bodies e.g. teeth from the wound, encouraging the wound to bleed, thorough irrigation, advising appropriate analgesia and prescribing prophylactic antibiotics if the wound is less that 48 hours old for animal bites, less than 72 hours old for human bites. Refer to A&E for further assessment if wound closure is necessary. Consider the need for tetanus and rabies prophylaxis. NICE CKS. Bites – human and animal; updated October 2020. https://cks.nice.org.uk/topics/bites-human-animal/ Insect bites and stingsA puncture wound or laceration inflicted by an insect. Most insect bites reactions resolve quickly although more persistent reactions are likely with tick bites. Complications include secondary bacterial infection from scratching, fever and malaise, systemic toxic effects, serum sickness-like reaction (rare) and anaphylaxis. Diseases may be transmitted via an insect bite, e.g. Lyme disease and malaria NICE CKS. Bites and stings; updated 2020 https://cks.nice.org.uk/topics/insect-bites-stings/ LacerationsTearing or splitting of the skin caused by blunt trauma or an incision of the skin caused by a sharp object. The most common complication of lacerations is infection, but there may also be injuries to the underlying nerves, tissue and blood vessels. The risk of infection is increased by:
Lacerations NICE Clinical Knowledge Summaries https://cks.nice.org.uk/lacerations Injuries – otherFurther information is available on a range of injuries at NICE Clinical Knowledge Summaries – select from menu at https://cks.nice.org.uk/specialities/injuries/ SUTURINGSutures (stitches) are the most commonly used method of closing a wound, used after thorough irrigation, exploration and removal of debris. Absorbable sutures dissolve over time (about 2 weeks), non-absorbable sutures need to be removed. Other methods of wound closure include tissue adhesive and Steri-Strips Patient. Simple wound management and suturing; 2015 https://patient.info/doctor/simple-wound-management-and-suturing BURN, SUPERFICIALPink, with blisters, and painful. Skin blanches on pressure. Should heal in 10 days with no scarring. Generally caused by scalding, electrical flash burn, radiation (sunburn). Management aims
Refer the following burn injuries:
British Burn Association. National Burn Care Referral Guidelines https://www.britishburnassociation.org/national-burn-care-referral-guidance/ Practice Nurse featured article Dealing with emergencies: First aid in general practice Beverley Bostock-Cox PRESSURE ULCER (decubitus ulcer, bed sore)Caused by a combination of friction and pressure (and individual contributing factors). Management aims
NICE CG197 Pressure ulcers: prevention and management. Guideline and care pathway, 2014 https://www.nice.org.uk/guidance/cg179 Health Improvement Scotland. Pressure ulcer grading and excoriation tool; reviewed 2019. https://www.healthcareimprovementscotland.org/our_work/patient_safety/tissue_viability_resources/pressure_ulcer_grading_tool.aspx WOUND SINUS A discharging blind-ended track, extending from the skin surface to an underlying cavity or abscess, eg a pilonidal sinus. Management aims
DRESSING SELECTIONSelection of an appropriate dressing requires familiarity with:
Many products are specific to a certain type of wound (acute, chronic, traumatic) or stage of healing. Choice may also depend on patient preference/tolerance, site of the wound and cost. Clinicians must be able to rationalise their choice of dressing and course of action and justify dressing costs. A local formulary of preferred dressings may be provided. Ideal dressingAn ideal dressing keeps the wound:
It should:
For certain wounds, the ideal dressing will also:
Dressings availableA variety of dressings are available, including:
BNF Wound Management Products Advice on wound dressings https://bnf.nice.org.uk/wound-management/ |
|
 LEG ULCER REFERRAL INDICATIONS
LEG ULCER REFERRAL INDICATIONS