WOMEN'S HEALTHWomen’s health includes a wide range of focus areas, including contraception, cervical screening, gynaecology, breast cancer, ovarian cancer and other female cancers. General practice nurses have an important role in highlighting to women the benefits of routine screening programmes, and offering verbal and/or written information on health awareness, explaining what is normal and emphasising the importance of seeing a nurse or doctor early if they notice any abnormality or change. While women in the UK on average live longer than men, women spend a greater proportion of their lives in ill health and disability when compared with men. The UK Government has published a Women’s Health Strategy for England (July 2022), which aims to boost health outcomes for all women and girls, and sets out the approach to priority areas including:
Reproductive health affects both men and women, but the greatest impact of reproductive ill health is on women. The World Health Organization defines reproductive health as ‘a state of physical, mental, and social wellbeing in all matters relating to the reproductive system. It addresses the reproductive processes, functions and system at all stages of life. Reproductive health, therefore, implies that people are able to have a responsible, satisfying and safe sex life and that they have the capability to reproduce and the freedom to decide if, when and how often to do so.’ Department of Health & Social Care. Women’s Health Strategy for England; 2022. https://www.gov.uk/government/publications/womens-health-strategy-for-england/womens-health-strategy-for-england
BMA. Reproductive health and wellbeing – addressing unmet needs; 2018 https://www.bma.org.uk/media/2114/bma-womens-reproductive-health-report-aug-2018.pdf
Gynaecological issues
A full pelvic examination, including examination of the cervix, is recommended for women presenting with:
See also Cardiovascular disease, contraception, osteoporosis, sexual health, urinary tract infections BREAST AWARENESS/BREAST SCREENINGThe NHS Breast Cancer Screening Programme offers breast screening (mammography) every 3 years to women in the UK aged 50–69 years for the detection of breast cancer. Women in their mid-20s and onward are encouraged to be ‘breast aware’; the DH leaflet Be breast aware sets out a five-point code:
NHS Breast Screening Programme https://www.gov.uk/topic/population-screening-programmes/breast Public Health England. Breast screening: information leaflets https://www.gov.uk/government/collections/breast-screening-information-leaflets NHS. Be Breast Aware (patient information leaflet). https://www.bggp.co.uk/wp-content/uploads/2016/10/Be-Breast-Aware_leaflet.pdf NICE NG101. Early and locally advanced breast cancer: diagnosis and management; 2018 https://www.nice.org.uk/guidance/ng101 NICE CG164. Familial breast cancer: classification, care and managing breast cancer and related risks in people with a famiy history of breast cancer; 2013 (updated 2019). https://www.nice.org.uk/guidance/cg164 Breast cancerBreast cancer is the most common cancer in the UK population (15% of all new cancer cases in 2017). Treatment is surgical intervention (wide local excision, mastectomy, lymph node removal), chemotherapy and radiotherapy according to individual need. Patients should see a breast cancer nurse specialist, but may appreciate additional support with treatment side-effects and advice on post-mastectomy rehabilitation, e.g. breast prostheses, breast reconstruction.
Practice nurse featured articles Primary breast cancer: what do practice nurses need to know? Tessa Watts Secondary breast cancer: the role of primary care nurses. Tessa Watts Cervical cancerCervical cancer affects around 2,800 women each year in the UK. Second most common cancer in women under 35. Virtually all cancers of the cervix are caused by persistent infection with human papillomavirus (HPV), a virus transmitted by skin-to-skin contact in the genital area. Infection is common but for most women does not result in cervical cancer. Cervical cancer is detectable at an early stage by cervical screening, which saves thousands of lives each year. Girls in England aged 12-13 years are offered vaccination against the two most common types of high-risk HPV (HPV 16 and 18). Since 2019, HPV vaccination has also been offered to boys aged 12 - 13 (school year 8). Immunisation Human papillomavirus (HPV) Pupblic Health England https://www.gov.uk/government/collections/immunisation#human-papillomavirus-hpv Cervical screeningTo detect and prevent cervical cancer, cervical cytology (sampling of cells from the cervix) screening is offered to women in the UK as follows: • England: women aged 25-49 years every 3 years; women aged 50-64 years, every 5 years. Transmen (assigned female at birth) do not receive receive invitations if registered as male with their GP, but are still entitled to screening if they have a cervix • Northern Ireland: women aged 20-64 years, every 3-5 years • Scotland: women aged 20-60 years, every 3 years • Wales: women aged 20-64 years, every 3 years Knowledge of the link between HPV and cervical cancer has transformed cervical screening, which is now based on HPV screening. If HPV is not found, the individual will be offered a screening test again in 3 to 5 years, depending on age. If HPV is found, a cytology test is used as triage to check for any abnormal cells. If no abnormal cells are found, a follow up screen is arranged for 12 months' time to see if the immune system has cleared the virus. If abnormal cells are found, the individual will be referred to colposcopy. It is important to encourage women to attend for screening when invited, but in recent years uptake has been falling. There is evidence that the HPV vaccination programme has reduced cervical disease both in vaccinated and unvaccinated women in later life but around 2,600 women are diagnosed with cervical cancer in England, and around 690 deaths, every year.
Cervical cytologyThe traditional cervical screening technique of smearing cervical cell samples on a glass slide before fixing for microscopic examination (the cervical smear) has been replaced by liquid-based cytology. The new technique allows the sampled cells to be dispersed directly in preservative fluid; the sample can then be spun and treated to remove obscuring materials (blood, pus, mucus). This reduces the risk of an inadequate sample and hence the number of repeat screenings, and laboratories can return results more quickly. TrainingNurses and doctors who carry out cervical screening must be adequately trained, and update of skills every 3 years is mandatory. Cytology training is a fundamental part of the NHS cervical screening programme ReferralIf there are clinical features suggestive of cervical cancer, a smear is not required before referral. A previous normal smear should not delay referral if indicated. Consider urgent referral for women with persistent intermenstrual bleeding and normal pelvic examination Practice Nurse featured article The impact of Human Papilloma Virus on cervical screening Val McMunn Colposcopy Examination of the cervix at up to 10x magnification, with a binocular microscope. Women are referred for colposcopy following an abnormal cervical cytology result.
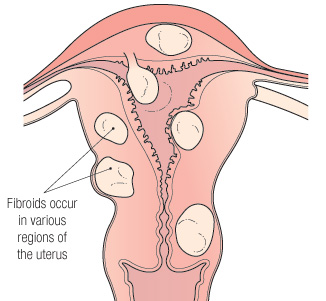
British Society for Colposcopy and Cervical Pathology (BSCPP) https://www.bsccp.org.uk FIBROIDS
Uterine fibroids affect more than 30% of women. They are benign tumours, ranging in size from that of a marble to that of a grapefruit, and originate from the smooth muscle layer (myometrium) and the accompanying connective tissue. Fibroids typically develop in the middle and later reproductive years, and tend to shrink with advancing age and after the menopause. Most fibroids are asymptomatic but others cause problems and may require treatment. Problems include: pressure on other organs, menorrhagia and intermenstrual bleeding, cramps, discomfort and urinary tract problems. Occasionally fibroids can affect a pregnancy. Fibroids are classified by their location, which often determines the appropriate treatment. Surgical removal of a fibroid is called a myomectomy. Fibroids may be discovered during a vaginal and pelvic examination. A suspected diagnosis can be confirmed using ultra sound. Further investigation may be with a hysteroscope (thin flexible telescope) inserted via the vagina or laparoscope (flexible tube with a light source and video camera) inserted via small abdominal incision. MENOPAUSEThe cessation of menses – the last menstrual period. In the UK menopause occurs generally at 51–52 years, following primary ovarian failure. A marker of the latter is increased production of follicle-stimulating hormone (FSH) and luteinising hormone (LH). Hormone levels do not decline gradually but sporadically, until they are too low to trigger ovulation. FSH can be measured but results are too variable to be a reliable test of menopause, which is generally diagnosed after 12 months of spontaneous amennorhoea in women ≥50 years, and after 24 months in women Postmenopausal women are at increased risk of CVD, breast cancer and osteoporosis. Symptoms, if present, are caused by reduced oestrogen levels, and may include:
Symptom management Menopausal symptoms may last for 2–5 years or for many years.
NICE Clinical Knowledge Summaries. Menopause; updated 2020. https://cks.nice.org.uk/topics/menopause/
Urgent referral is recommended for women with:
NICE NG12. Suspected cancer: recognition and referral https://www.nice.org.uk/guidance/ng12 Practice Nurse featured article Focus on women's health: The menopause Beverley Bostock-Cox Advising women on the menopause and diet Dr Frankie Phillips MENSTRUAL IRREGULARITIESNormal menstruation is the monthly cycle of blood loss per vagina that occurs from menarche to menopause; loss is about 25 ml per day for 4-5 days per month. Flow varies between individuals but tends to get heavier with age. To assess irregularities, a good detailed history of bleeding patterns is required. Physical examination and referral may be necessary, depending on the problem and the findings. Abnormalities in menstruation may include:
In women presenting with heavy menstrual bleeding, take a full blood count (FBC). Consider coagulation disorders in women with a history of heavy bleeding since menarche and/or with a history of coagulation disorders. Consider thyroid tests if other signs and symptoms of thyroid disease present. NICE NG88. Heavy menstrual bleeding: assessment and management; 2018 (updated May 2021) https://www.nice.org.uk/guidance/ng88 Practice Nurse featured article Management of menstrual problems Dr Mary Selby Practice Nurse Curriculum Module
VAGINAL BLEEDINGNon-menstrual bleeding should always be investigated. Women may present with:
Vaginal bleeding may be a sign of:
Patient. Intermenstrual and postcoital bleeding Professional reference; updated 2020. https://patient.info/doctor/intermenstrual-and-postcoital-bleeding NICE NG12. Suspected cancer: recognition and referral https://www.nice.org.uk/guidance/ng12 OVARIAN CANCERCommonly called the ‘silent killer’ because of ambiguous symptoms leading to late diagnosis. Around 6,800 women are diagnosed in the UK every year, and survival is seldom longer than 5 years after diagnosis. Key symptoms are now recognised as more common in women diagnosed with ovarian cancer, which should be considered if a woman has any of the following on most days:
If women present with any of these symptoms, they should be offered a blood test to measure the level of a protein called CA125, which is a marker for ovarian cancer, before being referred for an ultrasound examination. Occasionally urinary symptoms, changes in bowel habit, extreme fatigue or back pain may occur on their own or at the same time as those above. These symptoms may be vague and non-specific, and pelvic and abdominal examination may be necessary to determine possible causes. A symptom diary is available from Ovarian Cancer Action NICE CG122. Ovarian Cancer: recognition and initial management https://www.nice.org.uk/guidance/CG122 Ovarian Cancer Action https://ovarian.org.uk/ovarian-cancer/im-healthcare-professional/
Urgent ultrasound scan is recommended for palpable abdominal or pelvic mass. NICE NG12. Suspected cancer: recognition and referral https://www.nice.org.uk/guidance/ng12 PELVIC INFLAMMATORY DISEASE (PID)Fairly common bacterial infection of upper genital tract (uterus, fallopian tubes, ovaries). Usually begins as a chlamydia or gonorrhoea infection of the vagina or cervix; almost always sexually transmitted. Most frequent in sexually active women aged 15-24 years. Repeated episodes associated with an increased risk of infertility. NICE CKS. Pelvic Inflammatory disease; updated 2019. https://cks.nice.org.uk/topics/pelvic-inflammatory-disease/ See also Sexual health Polycystic ovarian syndrome (PCOS) Condition in which the ovaries have small cysts around their edges; symptoms include irregular or light periods, problems getting pregnant, weight gain, acne and excessive hair growth. PCOS is a leading cause of fertility problems, as women with PCOS fail to ovulate or do so infrequently. PCOS cannot be cured, but the symptoms can be treated. If not properly managed, PCOS can lead to problems such as type 2 diabetes and high cholesterol levels. NICE CKS. Polycystic ovary syndrome; updated 2018. https://cks.nice.org.uk/topics/polycystic-ovary-syndrome/ Patient. Polycystic ovary syndrome Professional reference; updated 2021. https://patient.info/doctor/polycystic-ovary-syndrome-pro URINARY TRACT INFECTIONSA UTI is an infection of any part of the urinary tract, i.e.
Urine is normally sterile (but asymptomatic bacteriuria is present in 20% of women) and most UTIs arise from E. coli, which normally lives in the colon. UTIs are:
And can be classified as:
The sites of infection are:
UTI symptoms and signsLower UTI (cystitis, urethritis) can present with dysuria, frequency, urgency, haematuria. The urine can be cloudy with an offensive odour. In older people, there may be generalised symptoms such as confusion and incontinence. Upper UTI symptoms (pyelonephritis) as for lower UTI symptoms plus suprapubic pain or tenderness, pyrexia and possible rigors. The patient is likely to be ill and might require hospital admission. Diagnosis may require collection of a mid-stream urine specimen (MSU). Vigilance necessary in children, the elderly and pregnant women. A UTI in a pregnant woman is more likely to spread to the kidneys. Advice to help prevent recurrent cystitis in women
Factors increasing risk of UTI
Public Health England. Diagnosis of UTI Quick Reference Guide for Primary Care; updated 2020 https://www.gov.uk/government/publications/urinary-tract-infection-diagnosisNICE CG54. Urinary tract infection in under 16s: diagnosis and management; 2007 (updated 2018). https://www.nice.org.uk/guidance/CG54 NICE NG109. Urinary tract infection (lower): antimicrobial prescribing; 2018. https://www.nice.org.uk/guidance/ng109
Practice Nurse featured article Urinary tract infections: assessment and management. Dr Gerry Morrow
NICE NG12. Suspected cancer: recognition and referral https://www.nice.org.uk/guidance/ng12 TOXIC SHOCK SYNDROME/TOXIC SHOCK-LIKE SYNDROMEMultisystem inflammatory response to exotoxins produced by Staphylococcus aureus and Streptococcus pyogenes bacteria. Can occur in anyone with a surgical or other wound, but many cases have been associated with women using tampons during menstruation. Incidence has declined since the early 1990s following changes in tampon manufacture, but infections not associated with menstruation have become more common as menstrual cases have declined. Symptoms may include:
Risk can be reduced by following common sense measures:
Advice for women:
Patient. Toxic shock syndrome Professional reference; updated 2020 https://patient.info/doctor/toxic-shock-syndrome-pro Toxic Shock Syndrome Information Service https://www.toxicshock.com VAGINAL DISCHARGENormal physiological vaginal discharge changes with the menstrual cycle. It is thick and sticky for most of the cycle, but becomes clearer and wetter around ovulation. Abnormal vaginal discharge is characterised by a change of colour, consistency, volume or odour, and may be associated with symptoms such as itch, soreness, dysuria, pelvic pain or intermenstrual or post-coital bleeding. Most commonly caused by infection e.g.
Non-infective causes include retain foreign body, inflammation due to allergy or irritation, tumours, atrophic vaginitis, cervical ectopy or polyps. Refer women with suspected PID (same day) or suspected trichomoniasis for genitourinary medicine clinic investigation. Arrange urgent admission for women with PID who are pregnant, pyrexial and unwell or unable to take oral fluids or medication. NICE Clinical Knowledge Summaries. Vaginal discharge, 2019. https://cks.nice.org.uk/topics/vaginal-discharge/ Patient. Vaginal discharge. Professional reference; 2015. https://patient.info/doctor/vaginal-discharge
|
|
 NICE NG12. Suspected cancer: recognition and referral
NICE NG12. Suspected cancer: recognition and referral