
Rabies: what general practice nurses need to know
Mandy Galloway
Practice Nurse 2026;56(2): online only
Since the death of a British woman from rabies in June 2025 there has been a surge in rabies post-exposure treatment requests and the Government has updated its advice about the risk of the disease and what to do before travel, and after exposure
Rabies is a viral disease transmitted to humans, usually via a bite or scratch from an infected animal.1 Dog bites and scratches cause 99% of cases of rabies, which is responsible for some 59,000 deaths every year: once the virus enters the central nervous system, rabies is invariably fatal.2,3
Rabies is a zoonotic viral encephalitis caused by infection with a lyssavirus. After initial exposure, the virus replicates within muscle tissue before advancing through the peripheral nervous system to reach the spinal cord and brain. Once in the central nervous system, the virus proliferates rapidly and subsequently spreads via neural pathways to various tissues, including the salivary glands. Death results from molecular-level neuronal dysfunction.1
The incubation period for rabies is typically 2–3 months but may vary from one week to one year, depending on factors including the location of virus entry and the viral load. Initial symptoms of rabies include generic signs such as fever, pain and unusual or unexplained tingling, pricking, or burning sensations at the wound site. As the virus moves to the central nervous system, progressive and fatal inflammation of the brain and spinal cord develops.2
Rabies has two forms: furious rabies causes hyperactivity, hallucinations, poor coordination, hydrophobia, and aerophobia, leading to death from cardio-respiratory arrest within days. Paralytic rabies begins with progressive muscle paralysis at the wound site, gradually leading to coma and death. This form is often misdiagnosed.2
The UK has been free from rabies in animals other than bats since 1902, making domestic infection extremely rare, but six cases of rabies acquired abroad were reported in the UK between 2000 and 2024.4 In June 2025, British traveller Yvonne Ford became the first person to die of rabies in the UK since 2018. She was scratched by a puppy in Morocco in February 2025, but only began to experience symptoms – including headache and paralysis – two weeks before her death. She did not seek treatment at the time of the initial injury because the scratch seemed so minor.5 Previously, a Scottish naturalist died following infection with the rabies-like virus, European bat lyssavirus, in November 2002, while volunteering on a bat research project.6
However, rabies deaths are preventable: effective vaccines are available to immunise people both before and after potential exposure.2
Prevention is crucial for travellers visiting countries where rabies is endemic, particularly in parts of Asia, Africa, and Central and South America.4 Vaccination is strongly advised for travellers planning to stay for over a month, engaging in outdoor activities, or travelling to areas with limited access to medical care.4
General practice nurses providing travel services have a crucial role to play in advising travellers of the potential risks and how to avoid them.7
RABIES IN NUMBERS
- 123 – number of years the UK has been rabies-free
- 4,743 – number of calls to RIgS related to rabies prophylaxis or post-exposure treatment
- 59,000 – annual number of deaths from rabies globally
- 99% – percentage of rabies cases caused by dog bites
- 100% – mortality rate once symptoms appear
RISK ASSESSMENT
An essential part of any travel consultation is the risk assessment that the health care professional must complete before advising on, or administering, any vaccines (or malaria prophylaxis).7
To determine whether a country is considered high risk for rabies, either consult the NaTHNaC Country Information pages at https://travelhealthpro.org.uk/countries or visit the A-Z list of countries and their category risk for rabies, last updated in May 2024, available at https://www.gov.uk/government/publications/rabies-risks-by-country .
Rabies is found on all continents except Antarctica, but the risk of human cases is highest where the virus circulates in dogs. However, rabies can be spread to humans from saliva from any infected mammal.1 Australia, the UK and parts of Western Europe are considered free of rabies in terrestrial animals, but lyssavirus (bat rabies) is considered an emerging public health threat.1
Consider also the remoteness of the travel destination, as it may be more difficult for the traveller to access appropriate care if they are exposed, and also activities in which the traveller intends to participate – for example, dogs will often chase runners or cyclists.8
PRE-EXPOSURE PROPHYLAXIS
The Green Book3 recommends pre-exposure prophylaxis (PrEP) for the following groups in the UK:
- Those working on rabies virus in laboratories
- People working in DEFRA-authorised quarantine premises and carrier
- People who regularly handle bats (including volunteers) in the UK
- Veterinary and technical staff who are at increased risk because of the nature of their employment.
The Green Book3 also recommends PrEP for people travelling outside the UK, including:
- Travellers to rabies endemic areas, especially if:
- Post-exposure medical care and rabies biologics are unavailable at the destination
- They are undertaking higher risk activities such as cycling or running
- They are living or staying at the destination for more than one month
Posology
Primary PrEP consists of three doses of rabies vaccine, given intramuscularly on days 0,7 and 28. The third dose can be given from day 21 if there is insufficient time before travel.1 Alternatively, where time before travel is limited, an accelerated course may be offered, with the three doses given intramuscularly on days 0, 3 and 7. New advice from the UK Health Security Agency and the Joint Committee on Vaccination and Immunisation on a two-dose pre-exposure regimen, 7 days apart, is expected.1
The World Health Organization favours moving from intramuscular (IM) administration to intradermal (ID) administration, which reduces the amount of vaccine necessary and the number of doses, thereby reducing costs without compromising safety or efficacy, and promoting patient adherence to the recommended regimen.2 However, it should only be administered by this route by practitioners experienced in ID injection technique.3
Rabies vaccines can be given at the same time as other vaccines, including other travel vaccines. The vaccines should be given at separate sites, preferably in different limbs. If given in the same limb, they should be given at least 2.5cm apart.3 If the general practice nurse is not a prescriber, the vaccine can be administered under a Patient Specific Direction (PSD) as patient group directions (PGDs) cannot legally be used for non-NHS funded or private services such as travel vaccinations.
A full course of pre-exposure rabies vaccine provides good protection for most people; for people who completed their primary rabies immunisation more than a year ago and are travelling again to a high-risk area can have a single booster dose.4
NHS provision?
Rabies vaccine for travel is not provided on the NHS, so if your practice does not offer private vaccination, patients should be advised to attend a private travel vaccination clinic, or a pharmacy with travel health services.8 Note, patients should be advised to allow at least 8 weeks before travel to ensure they can receive the complete course.
NHS regulations state that practices can charge NHS patients for ‘immunisations for which no remuneration is payable by NHS England and which is requested in connection with travel abroad.’9 In other words, practices can charge patients for travel vaccines that are not available on the NHS.
Patients who require vaccination because they are at risk because of their work, should be advised to discuss it with their employer. However, volunteers who regularly handle wild bats can be offered vaccination on the NHS.8
PATIENT EDUCATION
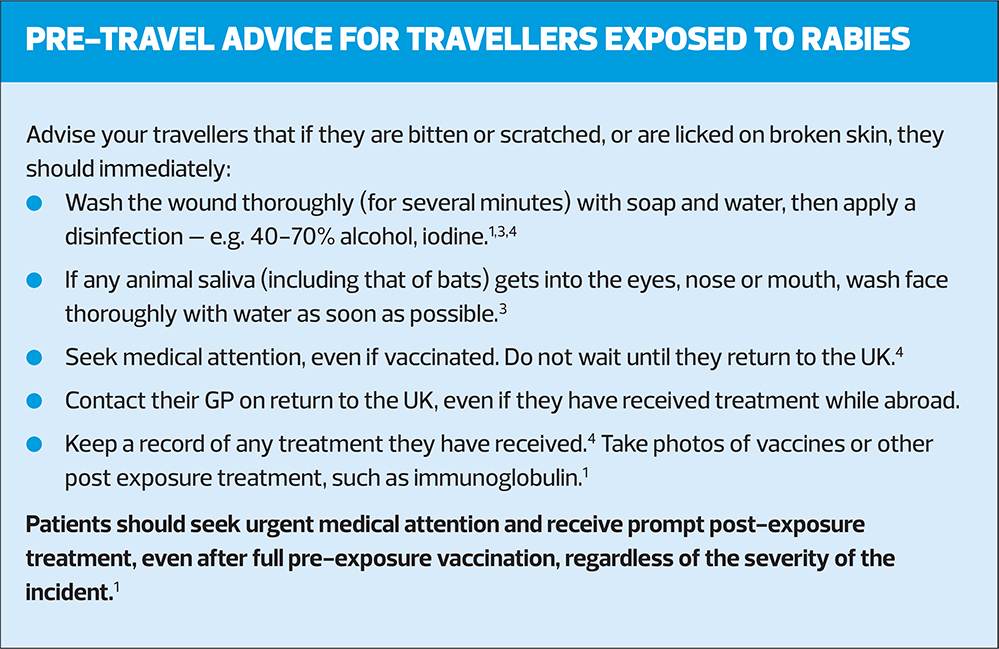
An important part of rabies protection is the provision of advice to travellers to help them stay safe.
This should include:
- Avoid contact with any wild animals (including bats), domestic animals or pets. Do not touch or feed animals, even within temples, zoos or sanctuaries.
- Don’t attempt to pick up an unusually tame animal/bat, or one that appears to be unwell: rabid animals may behave strangely but some may not show any signs that they are infected.
- Children are at higher risk of rabies because they often touch animals and might not report incidents. Advise patients travelling with children to inform them about animal risks and the importance of reporting bites, scratches, or licks. Closely supervise young children around animals and check for wounds if contact occurs.11
- Be aware that activities such as running and cycling can attract unwanted attention from dogs
- If a bat is found in the room of a sleeping traveller, or if they cannot give an accurate history of exposure, the person should be considered to have been exposed.
Overcoming objections
In her regular Travel Health Update for Practice Nurse, Jane Chiodini wrote: ‘The cost of a course of rabies vaccination is often considered “unaffordable” by some travellers and therefore the time and effort put in to educating on the topic can be limited. However, if there is contact with a mammal in a rabies-endemic area, the risk must be taken seriously and treatment given. If infection of the rabies virus occurs, then the outcome is almost always fatal. I feel travellers need to understand the risk, prevention measures and treatment pathways to make an informed choice prior to travel.’12
POST-EXPOSURE TREATMENT (PET)
If your patient has been exposed to rabies, contact the Rabies and Immunoglobulin Service (RIgS) urgently (See Resources).
Post-exposure management typically involves thorough wound cleansing and an assessment of risk to determine the need for appropriate post-exposure prophylaxis. Decisions regarding treatment and immunisation following potential rabies exposure are based on various factors, including the type of exposure, the animal species involved, geographic location, and the immune status of the individual affected.3
The UKSHA has issued guidance for healthcare professionals involved in the assessment and management of potential rabies exposures, to determine the combined country and animal risk.13
Risk assessment
Risk assessment should always be done, even if the exposure occurred many months or years previously.3
Consider:
- The site and severity of the wound
- Higher risk exposures are those with broken skin, including single or multiple transdermal bites, severe lacerations, or where mucous membranes or an existing skin lesion have been contaminated by the animal’s saliva or other body fluid. Intact skin is a barrier against infection
- Bites and severe lacerations represent a higher risk than scratches
- Bat bites from species in the UK are usually felt and not seen
- Bites to the head and neck exhibit a shorter incubation period than wounds to the limbs3
- The circumstances of the injury
- Species, behaviour, appearance and health of the animal involved
- Rabies can be transmitted by the saliva of any warm-blooded animal, including bats, monkeys and rodents as well as cats, dogs and foxes
- Animals behaving abnormally represent a higher risk of infection (but normal appearance and behaviour do not exclude rabies)
- Unprovoked bites carry greater risk than provoked bites3
- Vaccination status of the animal
- Country where the exposure occurred
- Vaccination status of the individual at risk.1
Each case requires a full risk assessment based on detailed information about the potential exposure, and, to avoid delay in post exposure treatment if this is indicated, general practice nurses dealing with such cases should try to collect as much of this information as possible, as soon as possible.3
This includes:
- Patient name, date of birth, age, address, and NHS number if possible
- Date of exposure
- Species and current health status of animal involved if known
- Country of exposure
- Category of exposure
- Site (on body) of exposure
- Whether the patient is immunosuppressed or has any allergies
- Any previous rabies vaccinations or immunoglobulin treatment
- Weight of the patient if human rabies immunoglobin (HRIG) is being considered.3
Treatment
As the incubation period for rabies can be prolonged, treatment should still be considered even if the interval from exposure is lengthy.3
The mainstay of rabies post-exposure treatment (PET) is rabies vaccine, with administration of HRIG directly in and around the wound, provided it can be given within the first 7 days following the incident or administration of the first dose of vaccine, or within one day of the second dose of vaccine.13
Vaccine should be administered as a 5-dose course, on days 0,3,7, 14 and 30. Antibody tests are recommended to confirm response to treatment at the same time as the fifth dose.1
HRIG may provide short-term immunity for the first 7 days before the vaccine takes effect.13 It is most useful if it is infiltrated at the wound site as it neutralises rabies at the wound site before the immune system can respond to the vaccine by producing antibodies.3 It should not be administered intramuscularly unless the patient is severely immunocompromised, a child, or has been exposed to a confirmed rabid animal, as the benefit of IM administration away from the site of the wound is likely to be negligible.3,13
In primary care, the first step in the event of a patient reporting potential exposure to rabies is to contact the Rabies and Immunoglobulin Service (RIgS) who will conduct a detailed risk assessment, provide clinical advice and issue immunoglobulins and anti-toxins where appropriate.
Immunoglobulins and anti-toxins are rare products that are centrally procured by UKHSA from a range of manufacturers. Stock is held both centrally, and at a number of locations distributed throughout the country.14
RIgS is a busy service; in 2024, there were 4,743 calls related to rabies prophylaxis or post-exposure treatment.
Since the rabies death reported in June 2025, there has been a surge in rabies post-exposure treatment requests, prompting the UKHSA to make recommendations to ensure the appropriate use of HRIG in the most efficient and clinically beneficial way.14
CONTACTING RIgS
- UKHSA. Rabies and Immunoglobulin Service (RIgS), Colindale: 0330 128 1020
- Scotland: contact hospital main switchboard for on call infectious diseases; a list of telephone numbers is available at: https://publichealthscotland.scot/population-health/health-protection/infectious-diseases/rabies/infectious-disease-contacts/
- Wales: contact the Wales Specialist Virology Centre at University Hospital Wales, Tel: 029 2074 2178; Out of hours: 029 2074 7747
- Northern Ireland: contact the Royal Victoria Hospital Pharmacy Department, Belfast on 028 9024 0503
- RIgS operates 7 days a week, from 9.30 am – 5 pm.
- An out-of-hours service is available to deal with the highest risk rabies exposures (injury to the head or neck or by an animal with confirmed rabies) for patients who have not already received one post-exposure dose of rabies vaccine.
- Requests for immunoglobulin/vaccine received Monday-Friday will be delivered to a named clinician by 2pm the next working day or more rapidly in specific urgent situations.14
CONCLUSION
The death from rabies of a woman in the UK in June 2025 drives home the importance of conveying the risk of rabies and the urgency of treatment following exposure to patients attending for travel advice. As a general practice nurse providing travel advice, it is beholden upon you to keep up to date with the latest Government advice on rabies, and to be familiar with sources of information on which countries are likely to pose the highest risk, such as Travel Health Pro. Nurses should also be aware of the protocols to follow if a patient in their care has been exposed to rabies – and practice receptionists should also be aware of the urgent nature of post-exposure treatment. Rabies in unvaccinated patients who do not receive appropriate PET is almost invariably fatal but it can be prevented with pre-travel vaccination, coupled with advice on how to minimise the risk of exposure.
RESOURCES AND FURTHER INFORMATION
NaTHNaC/Travel Health Pro https://travelhealthpro.org.uk/
A-Z list of countries and their category risk for rabies, https://www.gov.uk/government/publications/rabies-risks-by-country
UKHSA. The Green Book, Chapter 27: Rabies. https://www.gov.uk/government/publications/rabies-the-green-book-chapter-27
UKHSA. Rabies: summary of risk assessment and treatment. https://www.gov.uk/government/publications/rabies-post-exposure-prophylaxis-management-guidelines/rabies-summary-of-risk-assessment-and-treatment
Summaries of Product Characteristics for rabies vaccines licensed in the UK are available at https://www.medicines.org.uk/emc
UKHSA. Rabies Information for travellers. PDF. UKHSA gateway number 2024664. https://www.gov.uk/government/publications/rabies-risks-for-travellers
Patient. Rabies and rabies vaccine (information for patients). https://patient.info/travel-and-vaccinations/travel-vaccinations-leaflet/rabies-vaccine
NHS. Rabies. https://www.nhs.uk/conditions/rabies/
REFERENCES
- NaTHNaC. Rabies. https://travelhealthpro.org.uk/factsheet/20/rabies
- World Health Organization. Rabies; June 2024. https://www.who.int/news-room/fact-sheets/detail/rabies
- UK Health Security Agency. Rabies: the green book, chapter 27; last updated 2023. https://www.gov.uk/government/publications/rabies-the-green-book-chapter-27
- UK Health Security Agency. How to avoid rabies and what to do if you’re exposed while travelling; 18 June 2025. https://ukhsa.blog.gov.uk/2025/06/18/how-to-avoid-rabies-and-what-to-do-if-youre-exposed-while-travelling/
- Boyd R. Woman dies of rabies in Yorkshire after contact with dog in Morocco; 18 June 2025. https://www.theguardian.com/uk-news/2025/jun/18/person-dies-of-rabies-in-yorkshire-after-contact-with-dog-in-morocco
- Spooner MH. UK has first rabies death in a century. Can Med Assoc J 2003;168(3):331
- RCN Travel Health Nursing: career and competence development; 2023. https://www.rcn.org.uk/Professional-Development/publications/rcn-travel-health-nursing-uk-pub-010-573
- NHS. Vaccination – Rabies; Last updated 2023. https://www.nhs.uk/conditions/rabies/vaccination/
- The National Health Service (General Medical Services Contracts) Regulations 2015. (Amended 6 November 2023. https://www.legislation.gov.uk/uksi/2015/1862/regulation/25
- UKHSA. Rabies information for travellers; last updated November 2024. https://www.gov.uk/government/publications/rabies-risks-for-travellers/rabies-information-for-travellers
- Chiodini J. Travel Health Update; July 2014. Practice Nurse 2014;44(7):42
- UKHSA. Rabies: summary of risk assessment and treatment; 30 June 2025. https://www.gov.uk/government/publications/rabies-post-exposure-prophylaxis-management-guidelines/rabies-summary-of-risk-assessment-and-treatment
- UKHSA. Interim recommendations for human rabies immunoglobulin (HRIG) use; Updated June 2025. https://www.gov.uk/government/publications/rabies-post-exposure-prophylaxis-management-guidelines/interim-recommendations-for-human-rabies-immunoglobulin-hrig-use
- UKHSA. Rabies and Immunoglobulin Service (RIgS); Updated September 2025. https://www.gov.uk/government/publications/immunoglobulin-when-to-use/rabies-and-immunoglobulin-service-rigs
Related articles
View all Articles