Fitness to Fly
JANE CHIODINI
JANE CHIODINI
MSc(Travel Med), RGN, RM, FFTM RCPS(Glasg), QN
Dean, Faculty of Travel Medicine, RCPS(Glasg)
Founder and director of Travel Health Training
www.janechiodini.co.uk/
www.facebook.com/TravelHealthTraining
There are very few contraindications to air travel, but a ‘fitness to fly’ assessment sometimes needs to be performed and evidence of such may be required by an airline. Jane Chiodini looks into this complex area of travel health
As an increasing population choose to travel and the diversity of travellers increases, the mode of transport is important when planning a journey. This is particularly true when the traveller has a significant medical history that impacts on the journey risk. This article will focus on fitness to fly, although the traveller may find other challenges when travelling abroad by other modes of transport, such motion sickness with sea travel.
A review of tourism habits in the 1990s compared with more recent years identified a 68% rise in the number of holidays between 1996 and 2016, while the UK population increased by 12% in the same period.1 The twitter feed of the Civil Aviation Authority (CAA) informs us that there were 3.7 million requests for assistance at UK airports in 2018 – a rise of over 80% since 2010.2
An estimated 44,000 in-flight emergencies occur annually: 16 per 100 per million travellers, affecting about 1 in 600 flights. In-flight emergencies may be related to stress of travel, the cabin environment, or accident or trauma. The most commonly reported medical incidents during flight include syncope or presyncope, trauma and gastrointestinal, cardiac or respiratory ailments. Many airlines now carry automatic external defibrillators.3
The CAA is a public corporation, established by Parliament in 1972 as an independent specialist aviation regulator. In addition to licensing airlines and professional pilots, the CAA has a whole section on its website (https://www.caa.co.uk/passengers/) for the passenger in relation to issues before they fly: at the airport, on board, passengers requiring special assistance and resolving travel problems found. A section about fitness to fly is available and referral to the individual airline is advised. Detail is also provided about what an airline is and isn’t expected to provide, and is essential reading – especially for those who are more vulnerable, as it outlines the passenger rights and expectations and those of the carer if one is needed to accompany a passenger.
There are very few contraindications to air travel, but a ‘fitness to fly’ assessment sometimes needs to be performed and evidence of such may be required by an airline. These requirements may vary so it is always wise to check with the individual airline well in advance. For example, British Airways (BA) has a website page which outlines that for some medical conditions medical clearance before flying is required, for example:
- Recent illness, hospitalisation, injury or surgery
- Existing unstable medical condition
- Need for additional oxygen or use of medical equipment on board
- Travelling for medical reasons or treatment.
BA then provides a link to a downloadable medical information form – the MEDIF form. Part one requests information from the passenger, and includes their requests for any medical equipment, and Part two requires a doctor’s assessment.4 This is a service a GP can provide, but as such work will be provided privately, a fee may be requested. Such a service is also frequently provided within a private travel clinic. This form is then sent to the Passenger Medical Clearance team, which assesses the individual’s fitness to fly and advises if they will be able to travel, based on internationally accepted criteria from the World Health Organization.4,5 In some cases the medical clearance team may need additional information, or ask the passenger to travel with a medical escort or supplementary oxygen.
THE PHYSIOLOGICAL EFFECTS OF AIR TRAVEL
Hypoxia
An aircraft cabin pressure is usually maintained at 6000 – 8000 feet above sea level.5 The arterial oxygen saturation will fall to around 90% (Normal blood oxygen levels in humans are around 95–100 % at sea level). Because of this, less oxygen is taken up by the blood but this degree of hypoxia is well tolerated by the majority of travellers. Those who would be affected include people with cardiac and respiratory disease, people with haematological problems such as anaemia and, in particular, those with sickle cell anaemia. However, the majority of passengers with such problems may overcome this by using oxygen during the flight. Provision of supplementary oxygen needs to be arranged prior to travel and some airlines may charge for the service.
Barometric pressure
As the aircraft climbs to its cruising level and the cabin pressure decreases, there will be an increase in gas expansion in body cavities by as much as 30% and similarly, on descent in altitude, pressure increases and cause contraction of gases.6 If the gas is trapped and unable to expand freely within body cavities, problems may result causing barotrauma. This is most commonly experienced as ear ache in travellers who have upper respiratory tract infections – which are not of themselves usually dangerous. While ear pain is common, there is also a – less common – risk of perforation of the eardrum.
More significant is the entrapment of air after recent surgery, particularly intra-abdominal, neurologic, intrapulmonary, or intraocular procedures, which may cause serious complications and medical advice needs to be sought prior to departure. The Centers for Disease Control and Prevention7 gives the following advice in relation to barotrauma:
- People with ear, nose, and sinus infections or severe congestion may wish to temporarily avoid flying to prevent pain or injury
- Oral or nasal decongestants may alleviate symptoms
- Travellers with allergies should continue their regular allergy medications
- Travellers should stay hydrated to help avoid irritation of nasal passages and pharynx and to promote better function of the eustachian tubes
- Travellers sensitive to abdominal bloating should avoid carbonated beverages and foods that can increase gas production
- People who have had recent surgery, particularly intra-abdominal, neurologic, intrapulmonary, or intraocular procedures, should consult their physicians before flying.
Humidity and hydration
The aircraft cabin will have very low levels of water vapour and as a result the humidity levels in the cabin are typically in the range 10 to 20% compared with that in buildings, which is in the order of 40% to 50%.8 A low humidity in the aircraft cabin does not result in dehydration but dryness of the pharyngeal membranes, mucous membranes of the lips and tongue can lead to a sensation of thirst. Alleviate dry skin by using aqueous moisturising creams. Drying of the cornea can also create problems for the contact lens user and moisturising eye drops may help, but for the individual who is prone to developing dry eyes, it would be advisable not to use their contact lenses during a long flight.
Jet lag
The disruption of the circadian rhythm, particularly on a long distance flight can be very disruptive in the healthy traveller. It may be even more troublesome when regular medication is required e.g. the person with insulin-dependent diabetes.
Venous thromboembolism (VTE)
On a long distance flight (more than 4 hours), travellers may sit in a cramped space and have less opportunity to get up and exercise than in normal daily living. A risk of VTE will be greater in older travellers, pregnant women, those with a previous history of VTE or recent surgery, those with certain blood clotting disorders, malignancy, certain cardiac conditions and those taking oestrogen-containing medicines. Such travellers should consider the use of properly fitted compression socks. Low molecular weight heparin therapy may be recommended for those at particular risk. Aspirin is not recommended for the prevention of VTE during travel. To reduce the risk of VTE, travellers should regularly mobilise their legs by getting up and walking around the cabin where possible, or flexing and extending their ankles.9 See also the NICE CKS module on DVT prevention at https://cks.nice.org.uk/dvt-prevention-for-travellers#!scenario
IDENTIFYING RISKS IN THOSE WITH MEDICAL CONDITIONS
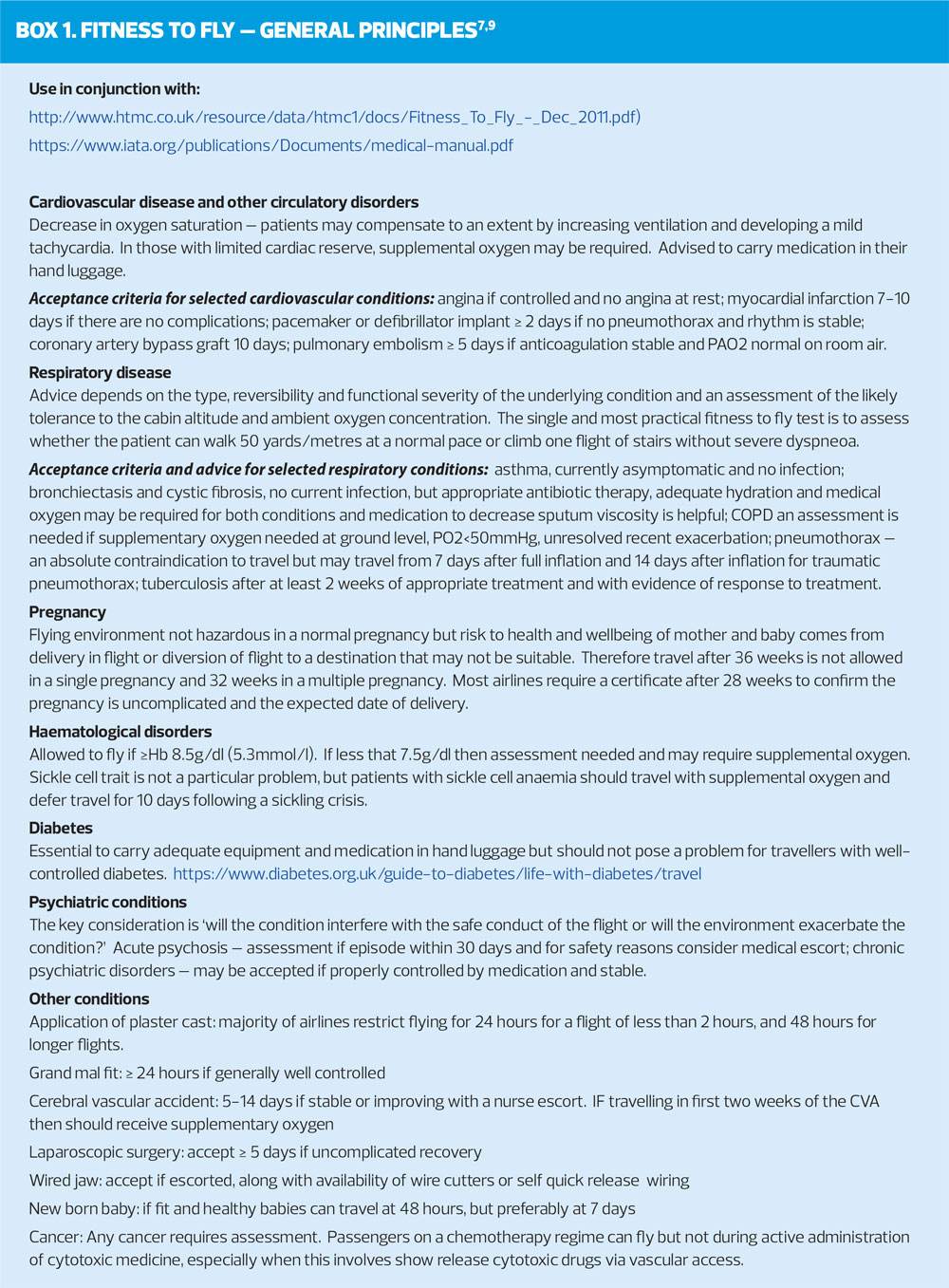
Greater detail on the specifics of fitness to fly are contained in Guidance for Healthcare Professionals on the CAA website at https://www.caa.co.uk/Passengers/Before-you-fly/Am-I-fit-to-fly/Guidance-for-health-professionals/Assessing-fitness-to-fly/. Within this section information is included for cardiovascular disease, diabetes, haematological disorders, pregnancy, psychiatric conditions, respiratory disease and surgical conditions. It is the physiological impact of airline travel that can effect some of these conditions and an understanding of their influence is important. The International Air Transport Association (IATA) is the trade association for the world’s airlines, representing some 290 airlines or 82% of total air traffic. It supports many areas of aviation activity and help formulate industry policy on critical aviation issues. IATA has a medical manual which details greater specifics on individual medical conditions, the assessments required and outlines acceptability of the individual traveller’s fitness to fly. Box 1 outlines some of the general principles that may impact a traveller, based on the information within these two documents, but the documents themselves should be accessed for complete information.8,10
CONCLUSION
Fitness to fly is a wide reaching and complex area of travel medicine. Awareness of good resources and guidelines is essential to direct potential travellers to seek advice and allow them to travel abroad with limited risk.
With the commercial launch of sub-orbital flight for science and tourism announced on a government website earlier this year at https://www.gov.uk/
guidance/how-we-are-promoting-and-regulating-spaceflight-from-the-uk who knows what the fitness to fly advice will need to cover in the future!
REFERENCES
1. Office for National Statistics. Holidays in the 1990s and now https://www.ons.gov.uk/peoplepopulationandcommunity/leisureandtourism/articles/holidaysinthe1990sandnow/2017-08-07
2. Civil Aviation Authority. Posting 11 July 2019 at https://twitter.com/@UK_CAA
3. Suh KN, Flaherty GT. The Older Traveller in: Travel Medicine 4th Edition, Eds. Keystone et al. Elsevier 2019
4. British Airways: Medical Conditions and Pregnancy. Medical clearance – am I fit to fly? https://www.britishairways.com/en-gb/information/travel-assistance/medical-conditions-and-pregnancy
5. WHO. Travellers with medical conditions or special needs https://www.who.int/ith/mode_of_travel/travellers/en/
6. Civil Aviation Authority. The physiology of flight. https://www.caa.co.uk/Passengers/Before-you-fly/Am-I-fit-to-fly/Guidance-for-health-professionals/Physiology-of-flight/
7. Lippold SA, Objio T, Kozarsky PE. Air travel in CDC Health Information for International Travel 2018. https://wwwnc.cdc.gov/travel/yellowbook/2018/conveyance-transportation-issues/air-travel
8. Civil Aviation Authority. Assessing fitness to fly – Guidelines for medical professionals from the Aviation Health Unit, UK Civil Aviation Authority. https://www.caa.co.uk/Passengers/Before-you-fly/Am-I-fit-to-fly/Guidance-for-health-professionals/Assessing-fitness-to-fly/
9. NaTHNaC. General advice in travellers. https://travelhealthpro.org.uk/factsheet/30/general-advice-for-travellers
10. IATA Medical Manual June 2018, 11th Edition https://www.iata.org/publications/Pages/medical-manual.aspx
Related articles
View all Articles