Supporting patients with bronchiectasis
Samantha Prigmore RGN BSc, MSc Independent Consultant Respiratory Nurse
Practice Nurse 2025;56(2):26-30
This article was supported by the education provider, Rotherham Respiratory
Bronchiectasis is a relatively common condition that can significantly affect the quality of life of people living with it. Providing education and self-management strategies is crucial to help patients minimise the extent of progressive lung damage
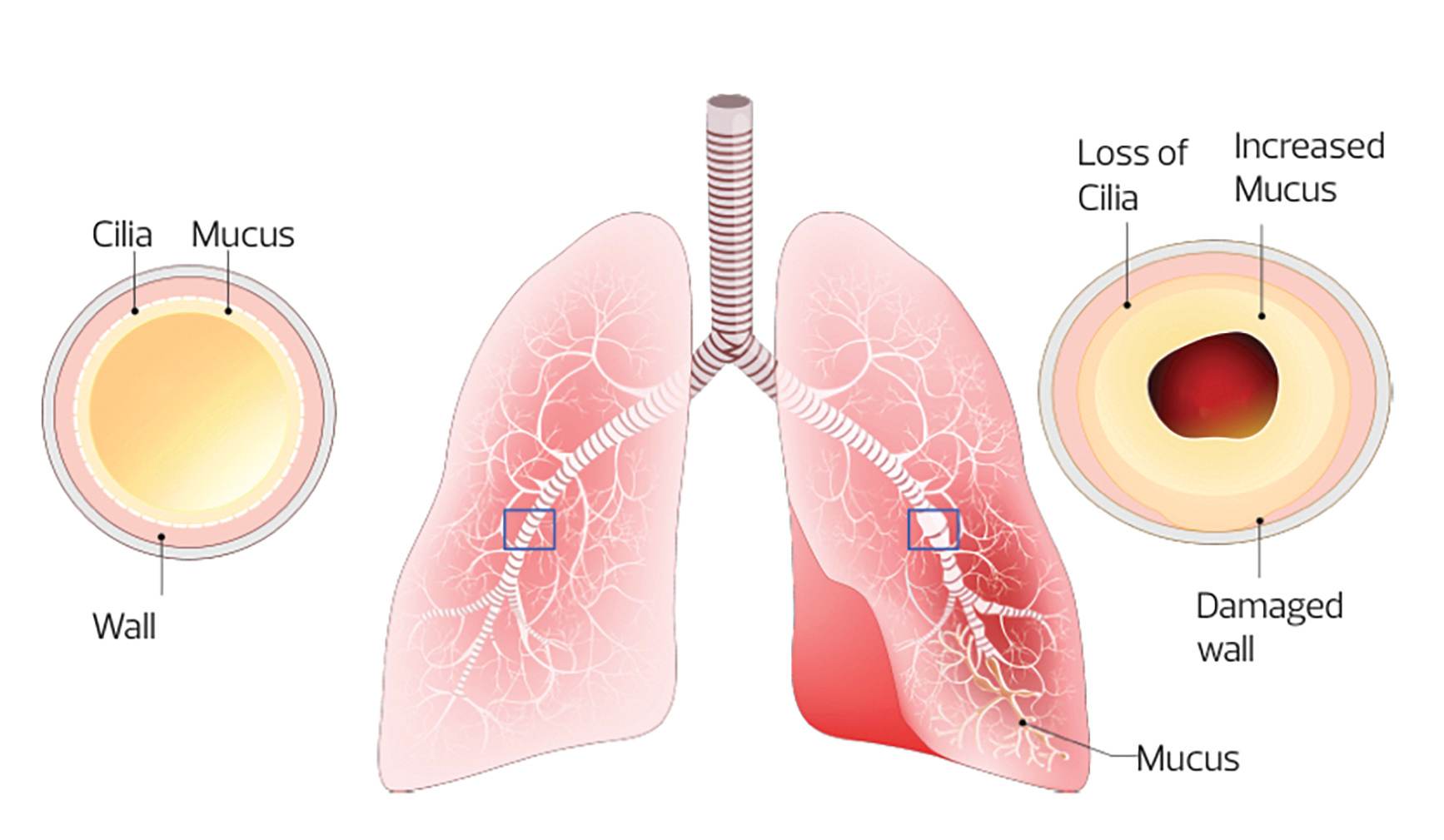
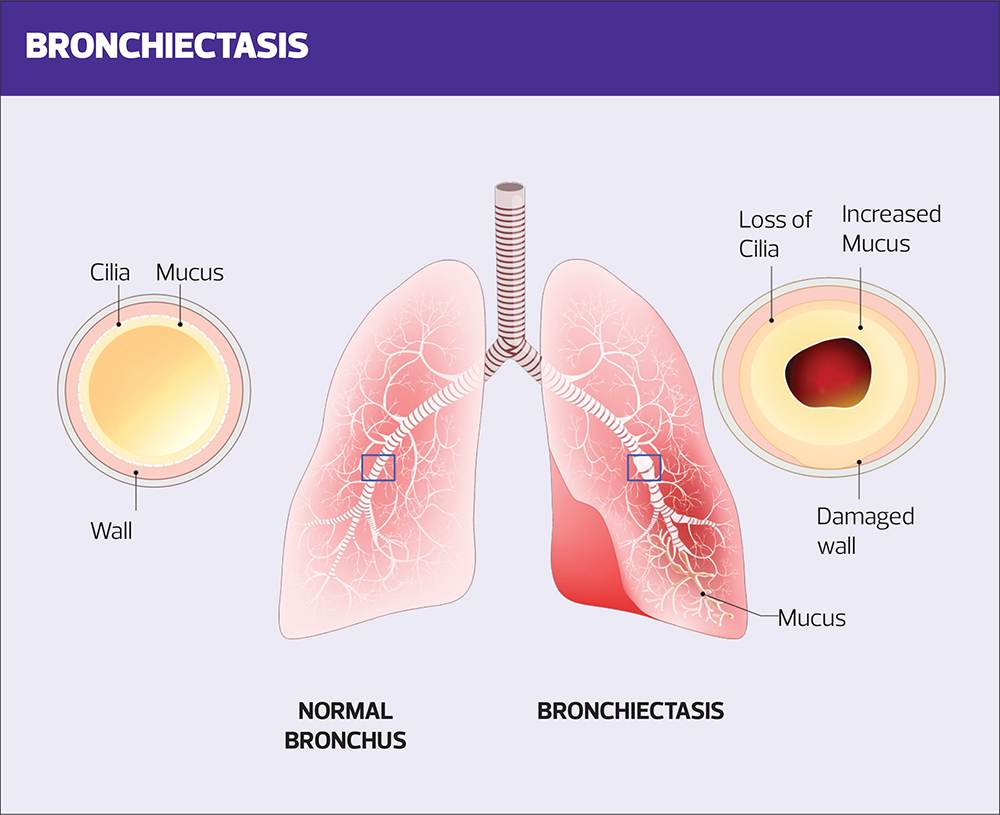
Bronchiectasis is a chronic condition in which irreversible damage to, and dilation of the bronchi, leads to symptoms of persistent or recurrent bronchial sepsis.1 The dilatation of the bronchi is irreversible, and results in the elastic and muscular tissue being destroyed by acute or chronic inflammation and infection. This impairs of the natural drainage of bronchial secretions which can become chronically infected resulting in mild to moderate airway obstruction. Unless appropriately managed, the combination of infection and chronic inflammation results in progressive lung damage.
Bronchiectasis is a relatively common respiratory condition affecting people of all ages. A GP practice of 10,000 patients will have around 50 adult patients with bronchiectasis, with 1% of people over 7- years of age living with the condition. It is more common is females, affecting 5.6/1000 females versus 4.9/ 1000 males.2
CAUSES
There are several known causes of bronchiectasis,3 where the individual is more prone to respiratory infection, or the condition affects the ability to clear secretions from the chest. These include:
- Post respiratory related infection e.g., pneumonia, whooping cough, measles, or mycobacterial infections.
- Presence of a muco-ciliary disorders e.g., primary ciliary dyskinesia, Kartagener’s syndrome, (comprising situs inversus, chronic sinusitis and bronchiectasis), Youngs syndrome (characterised by male infertility, bronchiectasis, and sinusitis)
- Obstruction of the airway lumen e.g., a foreign body, lung cancer or tuberculosis
- Cystic fibrosis which, while normally diagnosed in the first few weeks of life, can be missed and diagnosed later in life.
- Existing respiratory conditions e.g., chronic obstructive pulmonary disease (COPD), allergic bronchopulmonary aspergillosis (ABPA).
- Immune disorders e.g., hypogammaglobulinemia, HIV infection and cancers.
- A history of aspiration, including gastro-oesophageal reflux disease
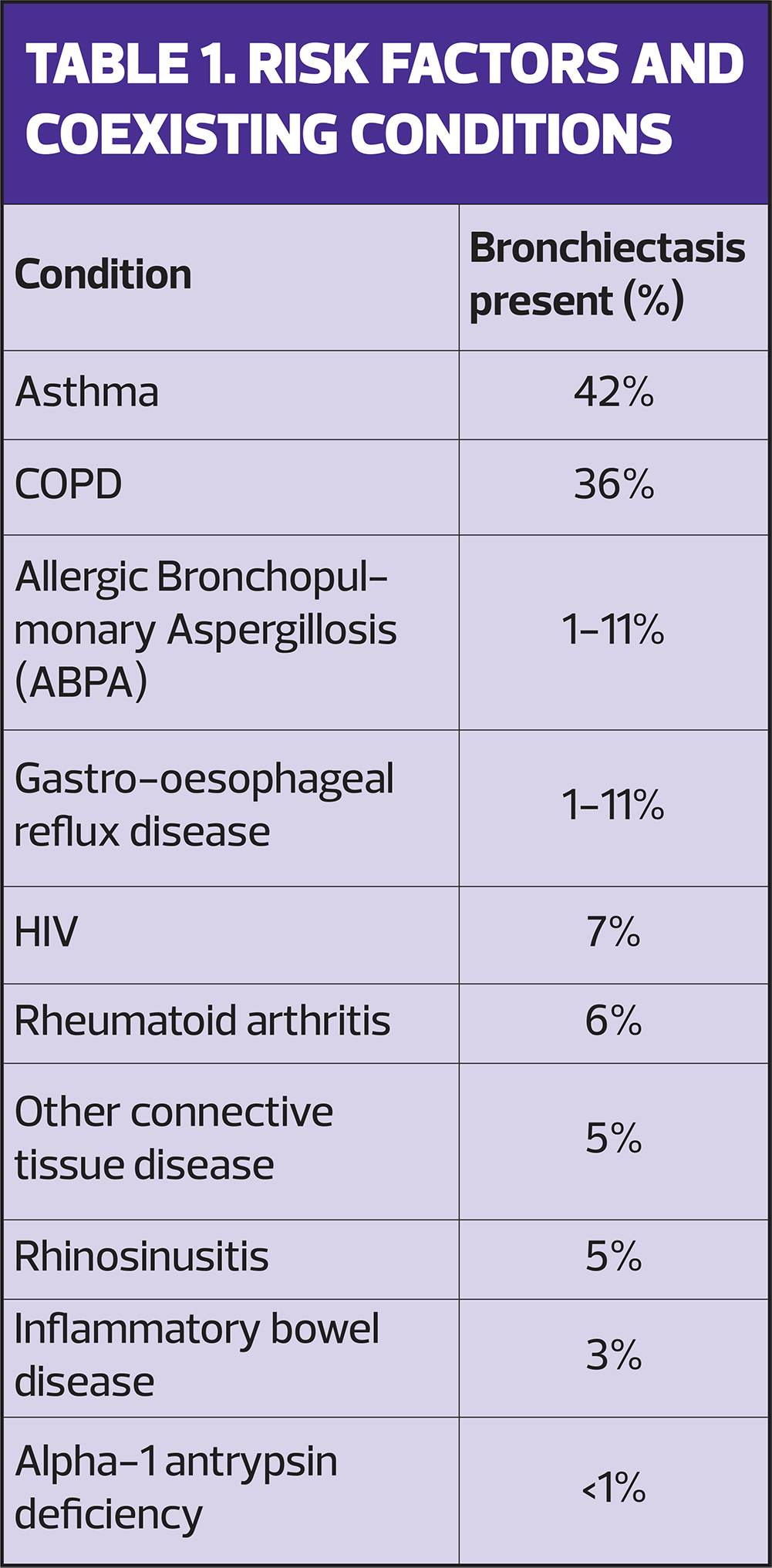
Despite the known causes of bronchiectasis, the underlying cause is idiopathic in 44% of cases.4 In addition to the known causes, there are several risk factors and health conditions which are associated with bronchiectasis (Table 1).
PRESENTATION
The overwhelming presenting symptom in patients with bronchiectasis is a chronic productive cough, present in 98% of people, but which patients may report having experienced for many years prior to being diagnosed with bronchiectasis. Experiencing chronic respiratory symptoms from childhood is not uncommon. Other common presenting symptoms include dyspnoea and fatigue.5
DIAGNOSIS
A diagnosis of bronchiectasis should be suspected in patients with a recurrent or persistent cough that has lasted for more than 8 weeks, and which features the production of purulent or mucopurulent sputum,1 with a lower index of suspicion if there are co-existing risk factors.6
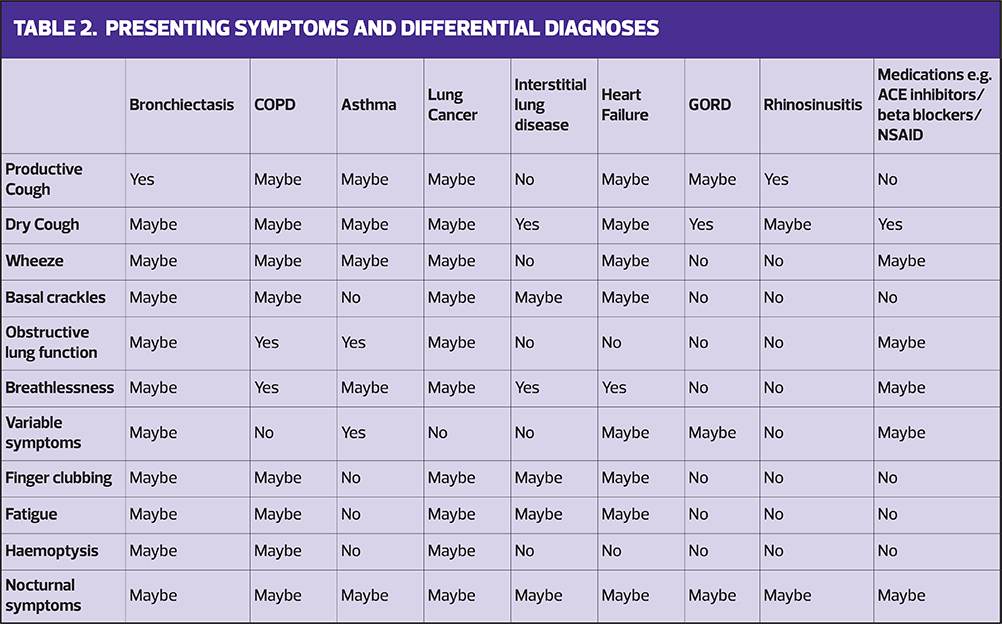
Diagnosis can be challenging due to similar presenting symptoms of other conditions and the presence of pre-existing conditions such as COPD and asthma. Table 2 highlights the differential diagnoses and the likely symptoms which may be present. It worth remembering that patients may have more than one condition driving their symptoms, and it is important to identify and treat the underlying causes.
MAKING THE DIAGNOSIS
A detailed clinical history and examination can help to determine the likelihood of bronchiectasis.
- Clinical examination may reveal inspiratory basal crackles, wheeze and finger clubbing.
- Clinical history should include presenting symptoms and past medical, drug and social history.
The duration and type of cough should be explored, along with the quantity, consistency, and colour of sputum production. Some patients will also report foul tasting sputum, especially during an infection. Breathlessness should be measured using the modified Medical Research Council (mMRC) breathlessness score.7 It is important to capture other symptoms, e.g., fatigue, incontinence due to coughing, to enable a holistic and comprehensive management plan.
Past medical history should include childhood illnesses such as measles or whooping cough, history of pneumonia, tuberculosis (TB) and chest or sinus infections.
A smoking history should be taken, and smoking cessation support offered to current smokers. Documenting the patient’s drug history is important, as common side effects of some medications may include breathlessness and cough.
It is important to record the frequency and severity of respiratory infections, as this helps to grade the severity of the disease.
It is helpful to explore vaccination history as this may highlight immune system deficits, which may be treatable. In addition, enquiring about fertility issues may identify ciliary function disorders.
Baseline investigations can help support the diagnosis of bronchiectasis, as well as exclude or identify alternative diagnoses. These should include:
- Pulse oximetry
- Hypoxia may be present in patients with severe bronchiectasis and should be appropriately managed.
- Routine blood tests
- Full Blood count to identify possible anaemia and white cell abnormalities.
- Renal and liver function tests as poor function is associated with risk of infection.
- Glucose and glycosylated haemoglobin (HbA1c) to exclude diabetes.
- Vitamin D level, as low levels of Vitamin D are associated with higher risk of infection.
- Sputum sample
- Sputum samples should be analysed for microbiology and cultured to identify bacterial and mycobacterial infection.
- Radiological tests
- Chest X-ray may identify infection and abnormalities. However, a normal chest X-ray cannot exclude the diagnosis of bronchiectasis.
- High Resolution Computerised Tomography (HRCT) scan is the gold standard test to confirm the diagnosis of bronchiectasis, although it may not be possible to arrange in primary care.
- Spirometry
- Spirometry is not particularly helpful in confirming the diagnosis of bronchiectasis but useful to exclude obstructive and restrictive lung conditions e.g., asthma, COPD and interstitial lung disease.
All patients with possible bronchiectasis should be referred to the respiratory specialist team to confirm the diagnosis, severity of the disease and develop a management plan for the patient.
LIVING WELL WITH BRONCHIECTASIS
Bronchiectasis is a long-term condition which can be managed in primary care. However, depending on the severity of the disease and treatment, some patients will continue to be followed up by respiratory specialists.
The main aims of management are to prevent further lung damage, maximise lung function, improve quality of life and reduce exacerbations. This will include identifying and treating any underlying causes, including optimising co existing lung conditions e.g., COPD or asthma.
Patients will need appropriate information and education about the condition and the important components of care, to help to prevent infections and ultimately further damage to their lungs. This should include an individualised self-management plan.
SPUTUM CLEARANCE
Respiratory physiotherapy is the cornerstone intervention to improve to the patients improve quality of life. This will include being taught and performing regular sputum clearance techniques, addressing breathlessness and reducing the risk of infections.
To reduce the risk of exacerbations, patients need to be able to effectively clear secretions from their chest. Therefore, patients should be referred to a specialist respiratory physiotherapist to be taught techniques to help mobilise and expectorate sputum.1 Sputum clearance techniques are effective, if practised regularly as part of a management plan. Many patients adapt quickly to including the techniques into their daily routines, but it is always sensible to check that they are undertaking them correctly.
Common techniques include active cycle of breathing technique (ACBT) and gravity assisted postural drainage to target specific lobes of the lung. There are excellent resources including videos, available at https://bronchiectasis.com.au/physiotherapy/techniques/gravity-assisted-drainage and https://www.acprc.org.uk/media/521payl5/gl-05acbt-1.pdf.
If sputum is difficult to clear, the use of an oscillating positive expiratory pressure (OPEP) device maybe recommended.The combination of positive expiratory pressure with high frequency oscillations helps with expectoration. There are contraindications to using OPEP devices, and therefore they should only be used following assessment and instruction from an appropriately trained healthcare professional.
Some patients may experience thick tenacious sputum.One of the commonest reasons for this is dehydration. Therefore, adequate fluid intake should be encouraged. Despite this, some patients may benefit from a trial of a mucolytic agent e.g., carbocysteine, or nebulised hypertonic saline to help reduce the viscosity of and loosen secretions.
BREATHLESSNESS
Breathlessness can impact significantly on patients’ quality of life. Guidelines recommend that patients should be referred to pulmonary rehabilitation if they have a mMRC >1, as itimproves quality of life breathlessness and reduces exacerbation rates.1
Unless a patient has a coexisting obstructive lung disease, there is little evidence for the routine use of inhaled corticosteroids, short acting beta-2 agonist (SABA), long-acting beta- 2 agonist (LABA) and long-acting anti muscarinic agents (LAMA). However, a trial of LABA/LAMA may be worth considering for significant breathlessness.6 In this situation, it is important to evaluate the effectiveness of inhaled therapy and discontinue it if there is no reported improvement in breathlessness.
EXACERBATIONS
Unfortunately, patients may experience exacerbations, and early intervention is important, as the frequency and severity of exacerbations have an impact on long-term outcomes.8
A bronchiectasis exacerbation is described as a deterioration in three or more of the following symptoms for at least 48 hours: cough, sputum volume and/or consistency, sputum purulence, breathlessness and/or exercise tolerance, fatigue and/or malaise, haemoptysis.1
The causes of exacerbations are multifactorial, including bacterial and viral exposure, inflammatory response and external environmental factors. People with chronic pseudomonas infection are more prone to infection and worse symptoms.8
The bronchiectasis severity indexhas been developed to assess the severity of the disease.9 The patient’s history, including age, weight, lung function, the number of lobes affected, frequency of severity of exacerbations, and pathogens identified, is used to calculate the severity of disease and associated risk of hospital admission and mortality.
MANAGEMENT OF EXACERBATIONS
An exacerbation can mild and managed with an increase in sputum clearance techniques, hydration and rest, but often will require a course of antibiotics. The British guidelines recommend a two-week course of antibiotics and provides guidance of choose of first- and second-line choice of antibiotics.1 For some patients, it may be appropriate to have an emergency course of antibiotics at home to commence if required, with clear guidance on when to start it.
Clinical assessment will determine the severity of exacerbation and ensure appropriate place of care, and additional community-based support, including referral to respiratory physiotherapy to aid sputum clearance, may be beneficial.
Indications for assessment in secondary care include:10
- Significant co morbidities and/or psychosocial factors that indicate that the patient cannot be managed safely in the community
- Potential requirement for intravenous antibiotics
- Signs of cardiorespiratory failure or sepsis, including;
- Cyanosis
- Confusion
- Marked breathlessness or laboured breathing
- Peripheral oedema
- Pyrexia (< 38oC)
Seek specialist advice from your local respiratory team if a patient is not improving following repeated courses of antibiotics, presence of pathogens in their sputum which are resistant to available antibiotics, or if they are unable to tolerate oral antibiotics.
It is important that all patients, and their care givers, are aware of when to seek advice and guidance during exacerbations and when to seek further advice and assessment.
Reducing the risk of infections is vital and therefore patients should be offered, and encouraged to have, the pneumococcal and annual influenza and COVD vaccinations, in line with current guidance. It is sensible to provide tips on reducing exposure to viruses, such as hand hygiene, and avoiding contact with people with coughs and colds.
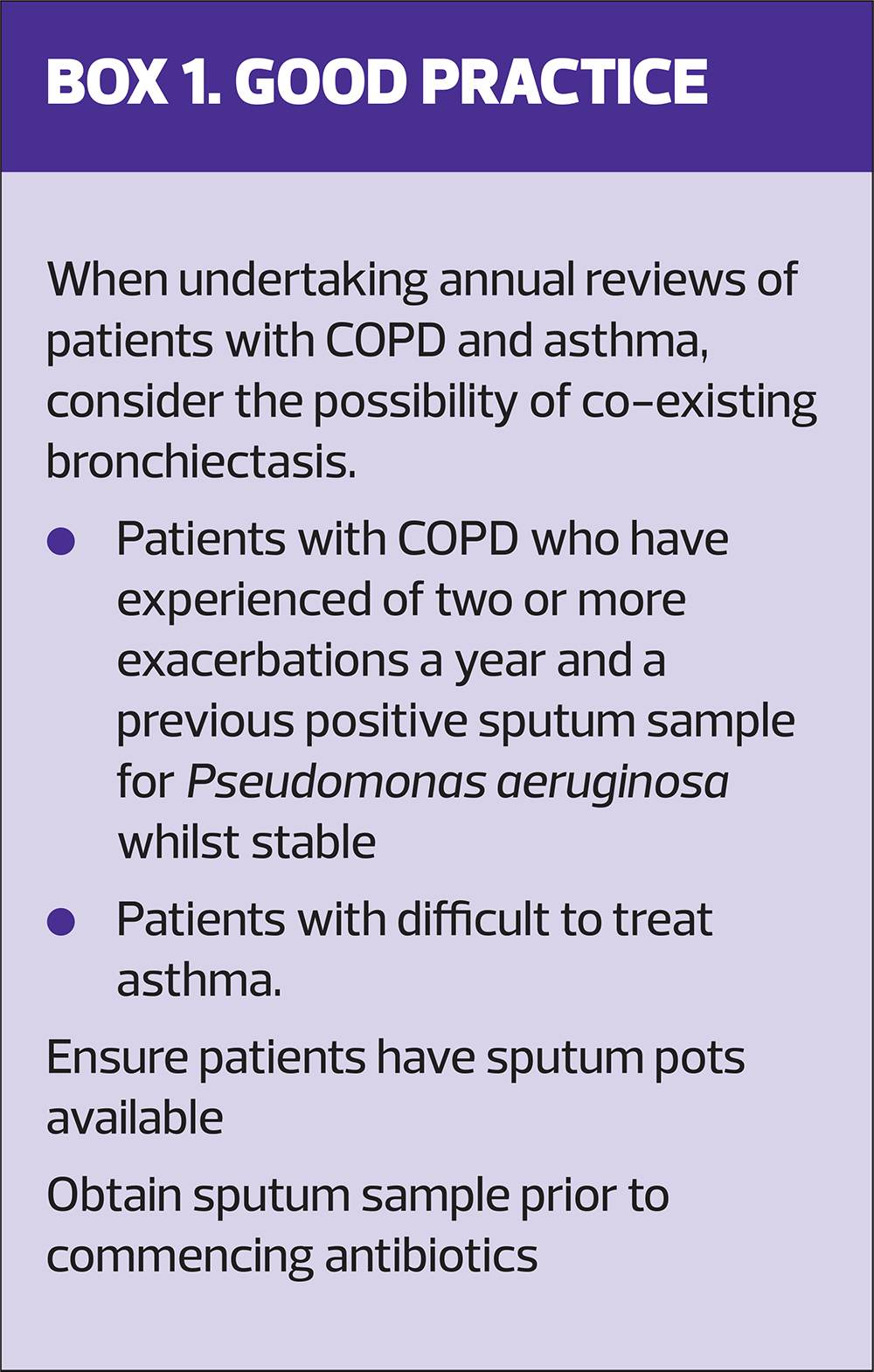
Patients who experience three or more exacerbations a year may benefit from prophylactic antibiotics e.g., azithromycin, or nebulized antibiotics to reduce the frequency of exacerbations, and they should be referred for specialist review.
SELF-MANAGEMENT PLANS
Although there is insufficent evidence to demonstrate the benefits of self-management plans for patients with bronchiectasis,11 guidelines recommend that they are considered, to enable early intervention when indicated. As with other long-term conditions, patient education is essential to enable self-management, and should cover routine treatment, respiratory physiotherapy guidance when well, how to recognise the signs of an infection or deterioration in their condition (exacerbation), and what actions they should take. These could be to make an urgent appointment for review, to provide a sputum sample or commence a course of antibiotics.
The management plan should be individualised, flexible and relevant to bronchiectasis.12
Asthma and Lung UK has developed several excellent resources, available at https://www.asthmaandlung.org.uk/healthcare-professionals/bronchiectasis. These include:
- An information booklet,
- A patient passport, which highlights what a patient should expect when diagnosed and ongoing management
- A digitised management plan
ANNUAL REVIEW
It is recommended that patients with bronchiectasis are reviewed at least annually.1
The review should include:
- Review of pneumococcal, annual influenza, COVID 19 vaccinations status.
- Record of exacerbation history and consideration of referral to respiratory specialists.
- Compliance with sputum clearance techniques and re-referral to specialist respiratory physiotherapy if necessary. OPEP devices should be replaced annually.
- Assessment of co-morbidities, such as asthma and COPD and optimise if necessary.
- Review and update of the management plan if required.
- Pulse oximetry and spirometry (for evidence of disease deterioration and existing airway disease)
CONCLUSION
Bronchiectasis is a relatively common condition which can significantly affect the quality of life of people living with it. Following the confirmation of the diagnosis, most cases can be managed in primary care. Providing education and self-management strategies, can help patients to identify the early signs of exacerbations, enabling early intervention and treatment.
References
- Hill A, Sullivan A, Chalmers J, et al. British Thoracic Society guideline for bronchiectasis in adults. Thorax 2019; 74 (Suppl 1):1–69doi:10.1136/thoraxjnl-2018-212463
- King P. The pathophysiology of bronchiectasis. Int J COPD 2009; 4:411-419 doi:10.2147/copd.s6133
- Quint J, Millett E, M Joshi, et al. Changes in the incidence, prevalence, and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. Eur Respir J 2016; 47(1):186–193. doi: 10.1183/13993003.01033-2015
- King PT, Holdsworth SR, Freezera NJ, et al. Characterisation of the onset and presenting clinical features of adult bronchiectasis. Respir Med 2006;100 (12):2183-2189doi: 10.1016/j.rmed.2006.03.012
- Gao Y, Guan W, Shao-xia L, et al. Aetiology of bronchiectasis in adults: A systematic literature review.Respirol 2016;21:1376-1383doi: 10.1111/resp.12832
- Gruffydd-Jones K, Keely D, Knowles V, et al. Primary care implications of the British Thoracic Society Guidelines for bronchiectasis in adults. NPJ Prim Care Respir Med 2019; 29: 24.doi: 10.1038/s41533-019-0136-8
- Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest 1988;93(3):580-6 doi: 10.1378/chest.93.3.580
- Choi H, Chalmers JD. Bronchiectasis exacerbation: a narrative review of causes, risk factors, management and prevention. Ann Transl Med 2023;11(1):25. doi: 10.21037/atm-22-3437
- Chalmers JD, Goeminne P, Alberti S et al The Bronchiectasis Severity Index: an international derivation and validation study. Am J Respir Crit Care Med 2014;189(5);576-585doi: 10.1164/rccm.201309-1575OC
- NICE Clinical Knowledge Summaries. Bronchiectasis: Scenario: infective exacerbation; 2025. https://cks.nice.org.uk/topics/bronchiectasis/management/infective-exacerbation/
- Kelly C, Grundy S, Lynes D, et al. Self-management for bronchiectasis. Cochrane Database Syst Rev 2018;2: CD012528. DOI: 10.1002/14651858.CD012528.pub2
- Kelly CA, Tsang A, Lynes D, et al. ‘It’s not one size fits all’: a qualitative study of patients’ and healthcare professionals’ views of self-management for bronchiectasis. BMJ Open Resp Res 2021;8:e000862. doi:10.1136/bmjresp-2020-000862
Related articles
View all Articles