Identifying and improving management of bronchiectasis
JANE SCULLION
JANE SCULLION
MSc, BA(Hons), RGN
Nurse Consultant,
University Hospitals of Leicester.
STEVE HOLMES
MMedSci, MBChB, FRCGP, DRCOG
GP, Shepton Mallet, Somerset.
PCRS-UK Education Lead
Mortality in patients with bronchiectasis is up to twice that of the general population, suggesting that this is a group who needs to be identified, correctly diagnosed, and for whom management should be improved
Bronchiectasis is defined in the British Thoracic Society (BTS) guideline as a progressive condition characterised by dilated, thick-walled bronchi and excessive sputum production.1 A recent European guideline,2 provides more clinically useful clarity on this definition, suggesting that: ‘clinically significant bronchiectasis, (is) defined by the presence of both permanent bronchial dilatation on computed tomography (CT) scanning and the clinical syndrome of cough, sputum production and/or recurrent respiratory infections’. The European guidance goes on to state that ‘radiological bronchiectasis may be evident in healthy asymptomatic individuals, particularly in the elderly and may occur, for example due to traction in interstitial lung disease.’ This is important as an analysis of bronchiectasis in primary care suggested that around two thirds of people with a specialist diagnosis of bronchiectasis at some point were asymptomatic over a three year retrospective review.3 This paper also identified that many (more than 80%) were managed solely in primary care, without specialist input – an area suitable for audit as these individuals still need to be correctly identified and coded so that they get appropriate management and referral when needed.
PREVALENCE
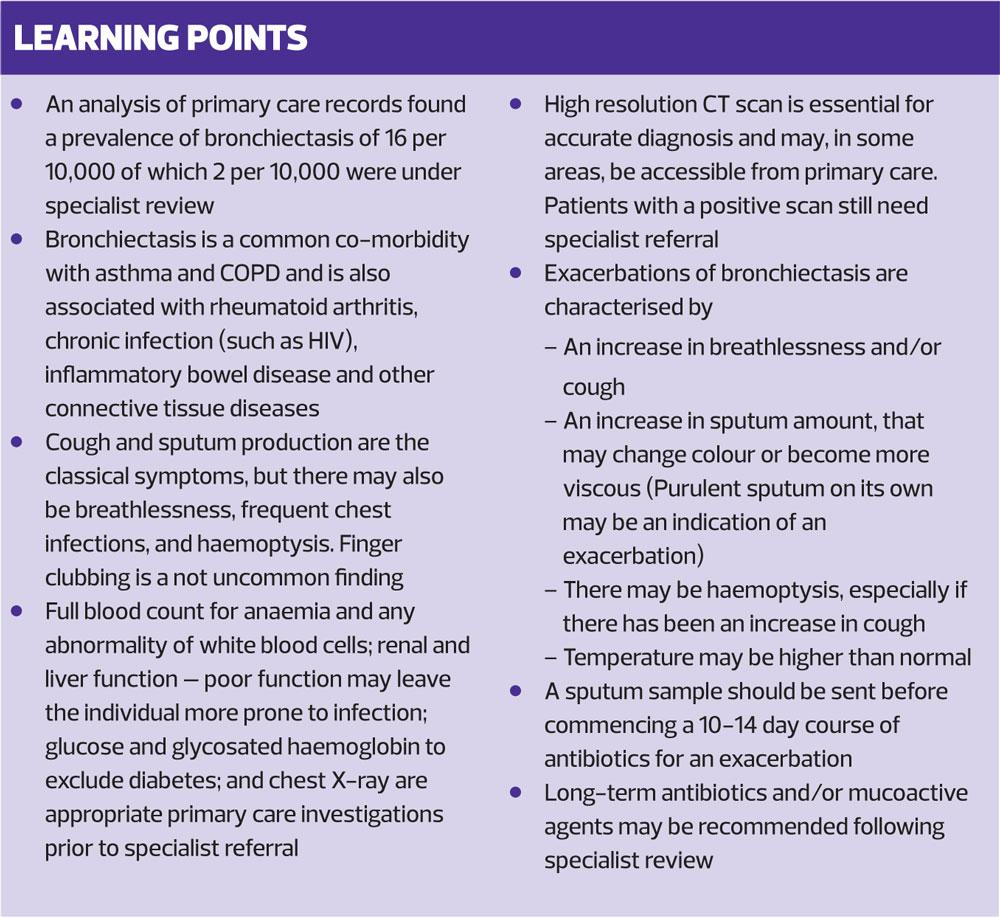
The estimated prevalence of bronchiectasis in the UK in 2013 was considered to be 57 per 10,000 in women, and 49 per 10,000 in men.4 However, this looked at any code for bronchiectasis and assumed the diagnosis was accurate, excluding those with a concomitant diagnosis of cystic fibrosis. An analysis of primary care records found a prevalence more in keeping with other research: 16 per 10,000 of which 2 per 10,000 were under specialist review.3 This fits with hospital admission rate data in the USA and New Zealand of around 1.6–2.6 per 10,000.
Quint4 found that 34% of people with bronchiectasis had no other significant co-morbidity, whereas the most common coded co-morbidities in the records were asthma (42%) and COPD (36%). Mortality in the Quint study appeared to be approximately twice that of the normal population, highlighting that this is a group of people we need to try to manage optimally.
PREDISPOSING CAUSES
The BTS guidance on bronchiectasis is currently being updated and the draft guidance,5 suggests that we should consider bronchiectasis in people with:
- COPD – studies show that a range of 25.6-69% of people with COPD have bronchiectasis on CT scan
- Asthma – a large study found 40% of people with difficult asthma had bronchiectasis on CT
- Rheumatoid arthritis – 4% to 58% of people with RA had bronchiectasis on CT
- Chronic infection (such as HIV) – appears to increase the risk of bronchiectasis
- Inflammatory bowel disease – increases risk of bronchiectasis
- Other connective tissues disease – Sjorgens syndrome, Marfan’s, systemic sclerosis, systemic lupus erythematosus and ankylosing spondylitis – also associated with an increased risk of bronchiectasis.
There are also a number of rare conditions that may leave an individual more likely to develop bronchiectasis, including those with ciliary dysfunction. Youngs syndrome (first described in 1970) links primary azoospermia with poor mucociliary clearance and may be associated with childhood mercury exposure (Pink disease) along with other rare childhood conditions such as primary ciliary dyskinesia.
PRESENTATION
Cough and sputum production are the classical symptoms of bronchiectasis, but there may also be breathlessness, frequent chest infections, and haemoptysis. The BTS guidance reminds us to be especially cognisant of these symptoms in people under 50, in non-smokers, and in people with other respiratory problems, specifically COPD and asthma.1
It is important to remember that haemoptysis should trigger referral for assessment of lung cancer, in England via a two week referral process rather than await routine specialist opinion and review.6 In addition, cough and sputum production are common with acute infections, and there are a variety of conditions that can present with breathlessness, hence careful clinical assessment is vital. Typically, in bronchiectasis, cough and sputum production is ongoing and chronic – and there is often a history of several presentations before a clinician considers the diagnosis.
Finger clubbing is not an uncommon finding in people with advanced bronchiectasis, but we should also think of carcinoma of the lung as a priority when clubbing is found. And, of course, there are other causes to think of too.
DIAGNOSIS
A detailed history and careful examination is required and NICE recommends that we refer all people with suspected bronchiectasis to a respiratory consultant for investigations to confirm the diagnosis and determine the underlying cause, and for initiation of appropriate treatment.7 However, in primary care it would be sensible to consider some basic investigations prior to referral if people present with chronic cough, sputum and recurrent infections, such as:
- Full blood count for anaemia and any abnormality of white blood cells
- Renal and liver function – poor function may leave the individual more prone to infection
- Glucose and glycosated haemoglobin – to exclude diabetes.
- Chest X-ray – this can exclude some infections and other causes, but it is important to remember that a normal chest X-ray cannot exclude a diagnosis of bronchiectasis and not all lung cancers will be visible on plain X-ray.
A high resolution CT scan is necessary to confirm the diagnosis of bronchiectasis. In many parts of the country, in light of the evidence for complex radiological investigations ordered by primary care having an improved pick up rate, the local radiologist will undertake a high resolution CT scan if a primary care clinician provides adequate information to suggest a diagnosis (or exclusion of) bronchiectasis (recurrent productive phlegm, recurrent chest infections and chronic sputum production). However, if the scan is positive specialist referral is still required.
The BTS guideline and NICE advise sputum culture, to look for any colonizing pathogens, remembering that pseudomonas aeruginosa isn’t often cultured in COPD,1,7 and a positive culture of pseudomonas (like MRSA and C. difficile) is often a result of frequent antibiotic usage. However, in many areas the current microbiological advice is not to culture sputum, except in very specific situations, as the interpretation is difficult.
Post bronchodilator spirometry, whilst widely available in primary care, is not particularly helpful. Normal, restrictive or combined obstructive/restrictive patterns of spirometry do not exclude or infer a diagnosis of bronchiectasis. There is also no recommendation to perform spirometry as part of the annual review of a patient with a confirmed diagnosis of bronchiectasis
Oxygen saturations should be checked,1 and in secondary care the gas transfer coefficient may be measured. This is the value of the transfer factor divided by the alveolar volume and is an expression of the gas transfer ability per unit volume of lung.8 If the patient has a disease that causes a decrease in lung surface area, or has had a lung removed, there is a decrease in transfer factor. Therefore, for people with bronchiectasis, a reduced transfer factor can indicate severity of disease.
NICE reminds us to think about documenting BMI and screen for anxiety and depression.7 The Bronchiectasis Severity Index (BSI) is a useful clinical predictive tool that can help identify those at risk of future mortality, exacerbations and hospitalization.9 http://www.bronchiectasisseverity.com/15-2/
The investigations advised by the European guidance after a clinical/ radiological diagnosis are:
- Full blood count with white cell differential. (Lymphopenia or neutropenia may suggest primary or secondary immune deficiency, while lymphocytosis may suggest secondary immune deficiency as a consequence of haematological malignancy)
- Serum immunoglobulins – total IgG, IgA and IgM (Low IgG, with or without low IgM or low IgA may indicate a defective antibody production, an important modifiable cause of bronchiectasis. Some 2–8% of patients with bronchiectasis have common, variable immune deficiency. In these cases, immunoglobulin replacement treatment can result in significant improvement in short and long-term outcomes.
- Testing for allergic bronchopulmonary aspergillosis (ABPA)
- Sputum culture to exclude bacterial growth and mycobacterial infection.
Other investigations may be considered, depending on the history.
For a generalist clinician it is appropriate to ensure the diagnosis is made by a specialist regularly involved in the management of active bronchiectasis – and the specialist may well decide to arrange follow up if the individual has active, clinical symptoms.
FOLLOW-UP AFTER DIAGNOSIS
We should refer people with three or more infective exacerbations a year. We should also refer people with fewer exacerbations if they are causing significant morbidity. Such individuals might be considered for long-term, prophylactic, antibiotic treatment, which requires initiation and monitoring by a specialist.
If the disease is stable with few exacerbations, follow-up will usually be exclusively in primary care, where an annual review is recommended. This should include:7
- Documentation of the number of exacerbations in the last year
- Level of breathlessness and consideration of referral to pulmonary rehabilitation
- Review of the self-management plan, the patient’s understanding of it and use of rescue medication
- Check that chest clearance is being undertaken and consider a referral or re-referral to a chest physiotherapist (though at times this may require specialist hospital referral)
- Offer of immunisation against Streptococcus pneumoniae and seasonal influenza
- Check vitamin D levels as a deficiency is associated with chronic bacterial colonisation and more severe disease 10
- Oxygen saturations.1
An annual sputum sample is also advised in people with continued purulent sputum in those with active disease (clinical symptoms). If a patient cultures Pseudomonas aeruginosa, opportunist Mycobacteria, or methicillin-resistant Staphylococcus aureus (MRSA), it would be appropriate to ensure that specialist help and active treatment is involved.
General health advice is also advisable and it would be appropriate to encourage three fundamental areas of a healthy lifestyle:
- Good diet
- Exercise
- Smoking cessation.
More specifically, chest clearance advice and airway clearance techniques by a trained respiratory physiotherapist, twice a week, may improve outcomes. Although access from primary care to such specialist treatment may be patchy at best, simple advice about chest clearance can still help. There is, however, strong evidence that pulmonary rehabilitation, tailored to symptoms, physical capability and disease characteristics can have a beneficial impact.
Both European and BTS guidance acknowledge that there are a large number of chest clearance devices available. The BTS updated, draft guidance,5 does not review the literature on these but provides a reference that has more information on the wide variety and current clinical recommendations by physiotherapists.11
Those with more severe disease may receive shared care or have the majority of their care managed by a specialist, with support from primary care.
Surgical interventions
The European guidance suggests that surgical interventions, usually lobectomy or partial lobectomy, should not be offered, except where the disease is localised and the individual experiences a high exacerbation frequency despite optimal treatment.
INFECTIVE EXACERBATIONS
In common with many respiratory disorders, people with bronchiectasis have exacerbations, and recognising an infective exacerbation is important. Signs of an exacerbation are:
- An increase in breathlessness and/or cough
- An increase in sputum amount, that may change colour or become more viscous
- There may be haemoptysis, especially if there has been an increase in cough
- Temperature may be higher than normal
Purulent sputum on its own may be an indication of an exacerbation.
Management
Many exacerbations can be managed at home with oral antibiotics. A sputum sample should be sent for culture and sensitivity testing before starting antibiotics, but you do not have to wait for the result before prescribing a 10-14 day course of anitbiotics.7 Any patient already taking long-term antibiotics should stop them until they have finished this course, and there may be a need to change the long term antibiotic afterwards. The European guidelines2 suggest a 14 day course of antibiotics, though they acknowledge the recommendation is conditional and based on very low quality evidence.
A sputum culture report may often suggest growth of a variety of potential pathogens – though often these can be normal commensals. The European guideline conditional recommendation, suggests that we treat a new isolation of Pseudomonas aeruginosa, but not other pathogens unless we are confident that the organism is causing significant infection.
The European guideline conditional recommendation, based on moderate quality evidence, is that long-term antibiotics be considered for people who have more than three exacerbations a year. Specialist colleagues may consider macrolides (azithromycin, erthryomycin) or inhaled antibiotics.
Oral or inhaled corticosteroids are not routinely advised by either the European or British guidance unless there is coexisting COPD or asthma.
European guidance suggests that specialist initiation of mucoactive treatment, e.g. expectorants, mucolytics, mucokinetic drugs and mucoregulators, may be considered in adults who:
- Are expectorating sputum, and
- Have a poor quality of life, and
- Have continued symptoms despite the used of standard airway clearance techniques.
They should not, however, be offered recombinant DNAse.
Hospital admission
NICE,7 recommends that we think about hospital admission in adults who:
- Are unable to cope at home
- Are cyanosed or confused.
- Have a respiratory rate of more than 25 breaths per minute
- Have signs of cardiorespiratory failure (such as marked breathlessness, rapid respiration, laboured breathing, cyanosis, or worsening peripheral oedema)
- Have a temperature of 38°C or more
- Are unable to take oral therapy
- Have failed to respond adequately to oral therapy.
- Have pleuritic pain severe enough to inhibit coughing and the clearing of secretions.
If the person deteriorates at any stage after starting treatment, they should be re-assessed to see if hospital admission is indicated.
CONCLUSION
In general clinical practice the patient who has a persistent cough, sputum production and regular chest infections should be considered potentially to have bronchiectasis. This is true if your patient has other respiratory conditions or a variety of rheumatic conditions or even if this appears to be without precedent.
Investigations involve routine blood testing, chest X-ray and a CT scan – and if the findings are positive or the test is not available, specialist care should be involved.
Many patients with bronchiectasis will have inactive disease, but it is important to treat those with active disease positively, with specialist medical, nursing and physiotherapist input.
The evidence from the literature indicates we need more research to be confident in our management, but we are moving forward. And it is clear that, as we do so, our patients will continue to need good, supportive care to enable them to reach the best possible outcomes.
REFERENCES
1. British Thoracic Society. Guideline for non-CF bronchiectasis. 2010. British Thoracic Society. https://www.brit-thoracic.org.uk/document-library/clinical-information/bronchiectasis/bts-guideline-for-non-cf-bronchiectasis/
2. Polverino E, Goeminne PC, McDonnell MJ et al. European Respiratory Guidelines for the management of adult bronchiectasis. European Respiratory Journal 2017; 50:1700629. http://erj.ersjournals.com/content/erj/50/3/1700629.full.pdf
3. Holmes S. Do the BTS guidelines on bronchiectasis resonate with a normal primary care population of people with bronchiectasis? RCP Annual Conference Glasgow 2012
4. Quint JK, Millett ERC, Miland J et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. European Respiratory Journal 2016;47(1):186-93
5. British Thoracic Society Guideline Development Group. British Thoracic Society guidelines for bronchiectasis in adults (draft) 2018 https://www.brit-thoracic.org.uk/standards-of-care/guidelines/bts-guideline-for-bronchiectasis-in-adults-public-consultation/
6. National Institute for Health and Clinical Excellence. Suspected cancer: recognition and referral. 2015. NG 12 https://www.nice.org.uk/guidance/ng12/resources/suspected-cancer-recognition-and-referral-pdf-1837268071621
7. National Institute for Health and Clinical Excellence. Clinical Knowledge Summaries. Bronchiectasis Feb 2016 https://cks.nice.org.uk/bronchiectasis
8. Holmes S, Scullion J. Diagnosis and management of patients with bronchiectasis Nursing Standard 2013;49;49-55
9. Chalmers JD, Goeminne P, Alberti S et al The Bronchiectasis Severity Index: an international derivation and validation study. American Journal of Respiratory and Critical Care Medicine 2014;189(5);576-585
10. Chalmers JD, McHugh BJ, Docherty C, Govan JR, Hill AT. Vitamin D deficiency is associated with chronic bacterial colonization and disease severity in bronchiectasis Thorax 2012;68(1):39-47
11. Flude LJ, Agent P, Bilton D. Chest physiotherapy techniques in bronchiectasis. Clinical Chest Medicine 2012; 33(2):351-61

Related articles
View all Articles