Gynaecological conditions
Dr Mike Wyndham is a GP in a suburban practice in Edgware Middlesex
Dr Mike Wyndham is a GP in a suburban practice in Edgware Middlesex
He has always been a keen photographer, and has been taking medical photographs for more than 25 years. He has been a regular contributor to the GP press and his work has also appeared in the British Medical Journal, The Pharmaceutical Journal and various medical text books
Women visit their GP surgery nearly twice as often as men, and gynaecological conditions are a common cause of presentation. Given the essential role of practice nurses in cervical cytology, here are some of the conditions that you may encounter in practice.
Ovarian Cancer
Ovarian cancer is the fifth most common cancer affecting women and predominantly affects women after the menopause. About 1 in 10 cases may have a genetic link. It can present with a range of symptoms including a distended abdomen which may relate to tumour growth or the development of ascites. Surprisingly, it may also cause symptoms that refer to the gastro-intestinal tract, i.e. bloating and extreme indigestion. CA125 is used as marker of ovarian cancer. However, not all tumours produce a raised test and the level may also be low in the early stages of development. Treatment will usually involve surgery and chemotherapy

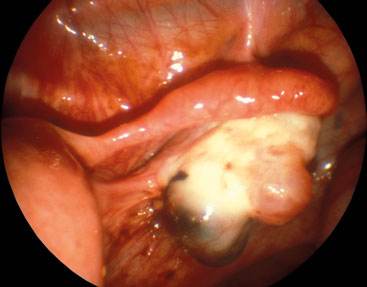
Infected Bartholin's Cyst
Bartholin's glands are located in the labia minora and the secretions produced help to lubricate the vagina. Problems with the gland usually occur between the age of 20-30 years. Presentation over 40 years of age is suggestive of malignancy. A cyst, which is usually painless, may develop in the gland. However, infection may occur which may cause symptoms such as dysparuenia and the development of a painful swelling. The cyst may discharge spontaneously. Infection is usually caused by organisms such as E. coli, Staphylococcus or Streptococcus. Less frequently, an infection may be caused by a sexually transmitted disease, most commonly chlamydia or neisseria. An infected cyst may be drained either by incision and passage of a catheter or by marsupialisation.

Endometriosis
Endometriosis describes the development of endometrium in places other than the uterus. Not only does this include the pelvis in places such as the ovary and utero-sacral ligaments, it may also be found anywhere in the body including lung, spleen, breast and kidney. There may be an associated family history. Presenting symptoms include chronic pelvic pain (which may or may not be cyclical), dysmenorrhoea, menorrahgia, pain on opening bowels, deep dyspareunia. Lung involvement may cause haemoptysis. Diagnosis in the pelvis may be made with the aid of ultrasound and MRI scans but laparoscopy provides the most information.
Urethral Caruncle
A urethral caruncle is a benign growth of the distal urethra, which is usually found in postmenopausal women. It may be asymptomatic but sometimes may be associated with dysuria or bleeding. It is therefore important that women who have recurrent dysuria have a pelvic examination. Urethral caruncles may be a cause of bleeding which is not surprising considering their red fleshy appearance. The differential diagnosis includes urethral prolapse which is more likely in the pre-menopausal women. Urethral cancer is rare. Treatment is relatively conservative with local oestrogen cream. Removal is only required when the lesion is large. Histology is required when the diagnosis is uncertain.

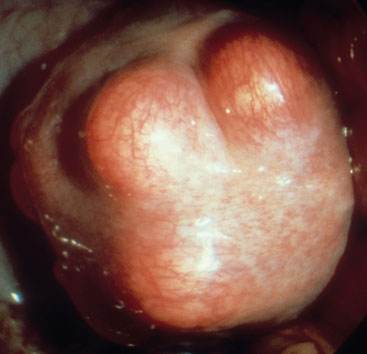
Fibroids
Fibroids are a benign growth of the uterine myometrium. They may grow in various places in the uterus: intra-mural - in the wall; subserosal - growing towards the pelvis; or sum-mucosal - growing into the uterine cavity. They may also grow from the cervix. They are more common in women of Africo-Caribbean extraction and more likely to be symptomatic in this group. For many, there may be no symptoms. However, they may cause menorrhagia (consider carrying out an FBC), undergo torsion causing pain, may be associated with infertility and may create pressure on the bladder affecting bladder emptying. During pregnancy, they may degenerate causing pain and fever.
Polycystic Ovaries (PCOS)
PCOS affects 5-10% women although some women will be symptomless. The main symptoms are: infrequent or absent periods, hirsutism, acne vulgaris, excess weight and infertility. Once the possibility of PCOS is considered, then investigations should include pelvic ultrasound and bloods for FSH, LH, testosterone and Sex Hormone Binding Globulin (SHBG). Once the diagnosis has been made then blood for fasting lipids and a glucose tolerance test should be completed in a caucasian woman with a BMI greater than 30 and a South Asian woman with a BMI greater than 25. Complications include metabolic syndrome with an increased risk of diabetes and subfertility. A recent publication suggested that pregnant women with PCOS are more likely to suffer with pre-eclampsia, diabetes and have a premature birth.

Related articles
View all Articles