
Bite-sized learning: Understanding EDS
Una O'Connor RGN MSc FHEA, Operational Manager, Learn With Nurses | Michaela Nuttall RGN MSC, Founder & Director, Learn With Nurses | Joanne Haws RN MSC, Clinical Director, Learn With Nurses
Practice Nurse 2026;56(2):9-10
Ehlers–Danlos syndrome is frequently under-recognised in primary care; general practice nurses play a key role in identifying hypermobility patterns and recognising vascular red flags.
INTRODUCTION
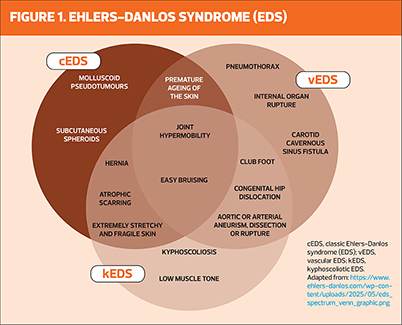
Ehlers–Danlos syndrome (EDS) describes a group of inherited connective tissue disorders characterised by joint hypermobility, skin hyperextensibility and tissue fragility. Hypermobile EDS (hEDS) is the most common subtype and is frequently encountered in primary care. EDS is a multisystem condition affecting the musculoskeletal, cardiovascular, gastrointestinal and autonomic nervous systems. Clinical presentation varies widely, and diagnosis may be delayed due to phenotypic variability and lack of definitive biomarkers for hEDS. Early recognition and appropriate referral are crucial to improve care coordination and long-term outcomes.
WHAT’S THE PROBLEM?
EDS comprises 13 recognised subtypes, ranging from relatively mild hypermobility presentations to rare, life-threatening vascular forms.1 While some subtypes are genetically confirmed and uncommon, others – particularly hypermobile EDS (hEDS) and hypermobility spectrum disorders (HSD) – are far more frequently encountered in primary care.
In a UK population cohort study conducted in Wales, the diagnosed prevalence of EDS and HSD was approximately 194 per 100,000 people (~1 in 500), although true prevalence is likely higher due to under-recognition.2
Diagnostic delay is common and may span several years. Patients often present repeatedly with chronic musculoskeletal pain, joint instability, fatigue and multisystem symptoms before hypermobility is considered. Limited awareness, absence of a confirmatory biomarker for hEDS, and symptom overlap with chronic pain and fatigue syndromes contribute to missed opportunities for earlier identification. As management is largely supportive rather than disease-modifying, timely recognition in primary care is essential to reduce avoidable morbidity and psychological distress.
DETECTION
Early detection of EDS relies on clinical awareness. GPNs are well placed to identify recurring patterns across consultations, including generalised joint hypermobility, recurrent sprains or subluxations, chronic widespread pain, easy bruising and delayed wound healing. Multisystem features such as orthostatic intolerance, gastrointestinal disturbance and persistent fatigue may also be present.
While hypermobility is common, clinicians should remain alert to features suggestive of rarer vascular subtypes. Recognition of hypermobility patterns in primary care has been highlighted as critical to reducing diagnostic delay.3 The Beighton score can support screening for generalised joint hypermobility. A detailed family history should include connective tissue disorders, early vascular events or unexplained sudden death. Identification of concerning features should prompt GP review and appropriate referral.
DIAGNOSIS
Although hypermobile EDS (hEDS) is the most common subtype encountered in primary care, rarer forms – particularly vascular EDS – require urgent recognition. Red-flag features include significant skin fragility, unexplained arterial or organ rupture, severe easy bruising, characteristic facial features (large, prominent eyes, a small chin, thin lips, hollowed cheeks), or a family history of early vascular events or sudden death. These findings warrant immediate medical review and referral to secondary care or clinical genetics, as complications may be life-threatening.
Diagnosis of hypermobile EDS is clinical and based on the 2017 International Classification criteria.1 Assessment requires evidence of generalised joint hypermobility, associated systemic features and exclusion of alternative connective tissue disorders. No confirmatory genetic test currently exists for hEDS. In contrast, classical and vascular EDS may be confirmed through molecular genetic testing where clinical suspicion is high.
MANAGEMENT
There is currently no disease-modifying therapy for EDS. Management is supportive and multidisciplinary, with primary care central to ongoing coordination.
GPNs play a key role in:
- Supporting joint protection and pacing strategies
- Encouraging appropriately tailored physiotherapy and strengthening programmes
- Monitoring wound healing and bruising patterns
- Supporting pain management plans
- Recognising associated conditions such as postural orthostatic tachycardia syndrome (POTS)
- Promoting psychological wellbeing and resilience.4
Smoking cessation, weight optimisation and general health promotion remain important components of care. Structured follow-up and coordinated referral to physiotherapy, pain services or specialist clinics can improve patient experience and reduce fragmentation of care.
REVIEW
Regular review supports early identification of deterioration and emerging complications. Follow-up should assess pain control, joint stability, functional capacity and psychological wellbeing. GPNs should remain vigilant for new vascular red-flag symptoms — including unexplained severe pain, sudden collapse, or unusual bruising — and ensure urgent escalation where required.
Ongoing education, validation of patient experience and support for self-management are central to effective long-term care.
References
- Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers–Danlos syndromes. Am J Med Genet C Semin Med Genet 2017;175(1):8–26.
- Demmler JC, Atkinson MD, Reinhold EJ, et al. Diagnosed prevalence of Ehlers–Danlos syndrome and hypermobility spectrum disorder in Wales: a national electronic cohort study. BMJ Open 2019;9:e031365.
- Hakim AJ, O’Callaghan C, De Wandele I, et al. Hypermobility spectrum disorders and Ehlers–Danlos syndrome in primary care: recognition and management. Br J Gen Pract 2021;71(708):e509–e511.
- NICE NG193. Chronic pain (primary and secondary) in over 16s: assessment and management; 2021. https://www.nice.org.uk/guidance/ng193
Related articles
View all Articles