COVID-19 and long term conditions: what’s the latest advice?
Mandy Galloway
Mandy Galloway
Editor
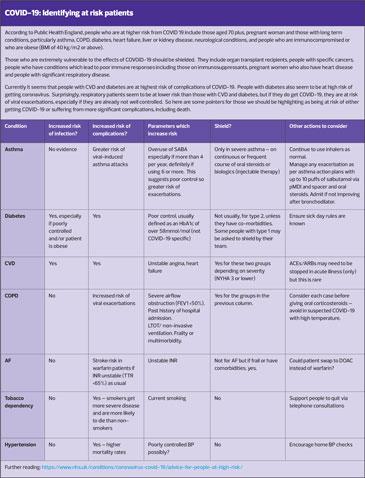
The number of confirmed cases of COVID-19 is increasing daily, and people with long term conditions are at increased risk of severe infection. As the scale of the outbreak in the UK has become apparent, organisations and charities representing patients with long term conditions, and the healthcare professionals with a special interest in these therapy areas, have been producing regularly updated advice.
RESPIRATORY CONDITIONS
Despite the fact that people who have underlying respiratory conditions are at increased risk of dying from COVID-19, most people with lung conditions experience mild symptoms and will fully recover. Continuing with normal medication regimes is key.
The Primary Care Respiratory Society (PCRS-UK) has produced ‘Pragmatic Guidance for crisis management of asthma and COPD during the UK COVID-19 epidemic’, which states: ‘Now, more then ever, it is essential we ensure patients with asthma and COPD are managed according to the latest clinical guidance.’
Asthma
PCRS states: ‘For patients with asthma, regular preventer inhaled corticosteroid (ICS) use remains central to the effective management of their condition. When taken as prescribed, ICS will reduce the risk of an asthma attack being triggered by a respiratory virus.
‘There is currently no evidence that ICS increase the risks associated with COVID-19 infection at the present time. Consequently, there is no change to the current recommendations for the use of ICS preventer medication for patients with stable asthma.’
PCRS member and GP Dr Katherine Hickman said: ‘I have never known so many asthmatic patients want the ICS that they stopped taking a few weeks ago. This is a great opportunity to hammer home the message about the importance of ICS as preventer medication.’
PCRS adds: ‘For patients presenting with an asthma attack, the shortest duration of increased ICS or oral corticosteroids to gain control of the asthma attack should be used. There is currently no evidence that ICS increase the risks associated with COVID-19 infection.’
Asthma UK recommends that patients ‘manage their asthma well to reduce the risk from coronavirus’
- Take preventer inhaler daily as prescribed
- Carry reliever inhaler in case symptoms flare up
- Use an asthma action plan
- Start a peak flow diary to keep track of symptoms, to help tell the difference between asthma and C19
- Stop smoking
- Follow advice on managing asthma when unwell, https://www.asthma.org.uk/advice/triggers/colds-and-flu/
Asthma UK has clarified which patients are classified as very high risk:
Any patient who is taking:
– Any biologic therapy, i.e. omalizumab, mepolizumab, reslizumab, benralizumab
– Oral corticosteroids every day
– Antibiotics (e.g. azithromycin) for asthma every week
– Tiotropium
– Combination inhaler containing high daily steroid dose
– High dose ICS + montelukast (See list at https://www.asthma.org.uk/advice/triggers/coronavirus-covid-19/ )
Or any patient who
– Has been admitted to hospital for asthma in the last 12 months
– Has ever been admitted to ITU for asthma
Asthma UK strongly recommends that such patients follow shielding guidelines, https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19
COPD
COPD is associated with a five-fold increased risk of severe COVID-19 infection, according to a rapid review published in the journal, Respiratory Medicine. Patients with COPD should therefore be encouraged to adopt more restrictive measures for minimising potential exposure to coronavirus and contact with suspected or confirmed cases of infection.
The Association of Respiratory Nurse Specialists (ARNS) recommends that current therapy should be continued, and antibiotics and oral steroids should be used in the same way as they would be under normal circumstances.
For patients with a COPD exacerbation, the PCRS says: ‘Consider carefully whether the benefits of oral steroids will outweigh the risks of worsening any viral illness. Before prescribing steroids, ensure you are advising that the control of symptoms with increased bronchodilation, breathing exercises and pacing, for example and where appropriate, can be highly effective. The absence of high blood eosinophil counts in past full blood counts (FBCs) suggests a COPD phenotype with less steroid responsiveness and here, avoidance of steroids is justifiable.’
Lippi G, Henry BM. Resp Med 24 March 2020; https://www.resmedjournal.com/article/S0954-6111(20)30081-0/fulltext
British Thoracic Society advice
Pulmonary rehabilitation classes stopped to reduce risk to patients and to allow staff redeployment to acute settings. Consider alternative methods of rehab such as online resources, e.g. British Lung Foundation https://www.blf.org.uk/exercise-video
Association for Respiratory Technology & Physiology (ARTP) has suspended lung function testing for all non-urgent patients to decrease the numbers of patients attending primary care. (Urgent includes inpatient cancer patients and preoperative patients for urgent surgery where lung function is essential).
Breathe Easy and other patient support groups should be suspended. (BTS)
Treating acute exacerbations of COPD: continue to treat with inhaled or oral corticosteroids according to NICE guidance. BTS states that there is no evidence to use or not to use oral or inhaled corticosteroids outside usual guidelines in COPD patients with COVID-19. Antibiotics should be issued only is suspicion of secondary bacterial infection.
DIABETES
The Primary Care Diabetes Society has produced an at-a-glance factsheet to help healthcare professionals manage patients with diabetes during the outbreaks.
It says: ‘While the majority of people who contract COVID-19 will experience only mild symptoms and make a full recovery, people with diabetes and/or other long term conditions are more likely to experience symptoms of greater severity.
‘Currently the spectrum of disease suggests that 81% of cases will be mild, 14% severe and 5% critical. The risk [appears] to increase in people aged over 70 years, particularly in those with comorbid heart disease, diabetes or respiratory disease.’
PCDS warns: ‘Be aware that people with diabetes, in addition to the expected respiratory symptoms of COVID-19, are also at increased risk of metabolic decompensation whilst trying to self-manage their diabetes at home.
- Ensure patients have adequate supplies of medication
- Ensure patients have an increased supply of monitoring equipment. This is especially important for those who require ketone monitoring equipment.
The factsheet also contains links to articles on how to advise on sick day rules, and using SGLT2 inhibitors safely during illness.
PCDS. COVID-19 and diabetes (factsheet). https://www.pcdsociety.org
Trend UK has produced updated Sick Day Rules booklets, available at: http://trend-uk.org/resources/
According to current guidance, most people with diabetes do not need to shield, unless they also have other comorbidities that make them extremely vulnerable. Instead they should follow advice to stay at home. People with diabetes should not be attending the practice (or pharmacy or hospital) if they have coronavirus symptoms even if they have an appointment. If they are currently having treatment for a foot or eye problem, and do not have coronavirus symptoms, they should keep their appointments. Most routine appointments will have been cancelled or postponed.
Diabetes UK has produced up-to-date advice for patients, available at:
https://www.diabetes.org.uk/about_us/news/coronavirus
NHS England has postponed the majority of activities related to the Diabetes Transformation Programme until Autumn 2020. Although NHS Diabetes Prevention Programme face-to-face services have been suspended, digital or remote delivery will continue to take place, and new referrals are still being accepted. The rollout of a new online service to support healthy living in patients with type 2 diabetes is being accelerated.
Type 2 Diabetes Prevention Week will not take place as planned from 20–26 April.
CARDIOVASCULAR DISEASE
The Primary Care Cardiovascular Society (PCCS) has ‘strongly recommended’ that patients prescribed ACE inhibitors or angiotensin receptor blockers (ARBs) should continue to take them.
The controversy was sparked when researchers speculated that these drugs may increase both the risk and severity of COVID-19, and suggested that clinicians should consider withholding ACEi and ARBs, and offer patients calcium channel blockers instead.
Their argument was that patients with cardiac disease, hypertension or diabetes who are treated with ACEi or ARB were at higher risk of severe COVID-19 infection because SARS-CoV-2 binds to target cells through angiotensin-converting enzyme 2 (ACE2), expression of which is increased in patients who are treated with these drugs.1
But the claim has been dismissed as a ‘premature hypothesis’ based on unadjusted observational data.2 The PCCS says reports in the press and on social media could lead to patients stopping their medications inappropriately, putting themselves at serious risk of a significant deterioration in the control of their blood pressure, heart failure or chronic or diabetic kidney disease.
PCCS says: ‘The concern about the safety of ACEi or ARB treatment has no sound scientific basis or evidence to support it. Indeed, there is evidence from studies in animals that these medications may be protective against serious lung complications in patients with coronavirus infection, but to date there are no data in humans.’
1. Fang L, et al. Lancet Respir Med 2020. ePub 11 March 2020. https://doi.org.10.1016/PII
2. Tignanelli CJ, et al. Lancet Respir Med 2020. ePub 26 March 2020. https://doi.org/10.1016/S2213-2600(20)30153-3
The European Society for Cardiology (ESC) has issued a statement reminding its members ‘not to forget the needs of patients with cardiovascular disease (CVD).’
‘During the current pandemic, more people will die of CVD than of COVID-19, but patients with CVD or CVD risk factors, such as hypertension, diabetes, and smokers, are more likely to die of COVID-19.’
The ESC says that hospital admissions of patients with acute coronary syndrome (ACS) have reduced drastically in the areas most affected by the pandemic. ‘Myocardial infarction patients are seeking medical help much later, or not at all, and more of them are admitted in cardiogenic shock.
‘It needs to be clear that “don’t come to hospital” does not apply to patients with ACS or other acute syndromes,’ said ESC President, Barbara Casadei.

Related articles
View all Articles