Coronavirus: what should general practice nurses do next?
Helene Irvine
Helene Irvine
Practice Nurse Adviser, Wessex LMCs
Deputy Clinical Lead, RCGP Primary Care Development
The first wave of COVID-19 may be easing but general practice is long way from getting back to normal. Here we look at activities that GPNs should be resuming – albeit in perhaps a different way from before the start of the pandemic
‘We must not return to where we were, but to where we want to be’
– Niall Dickson, chief executive, NHS Confederation
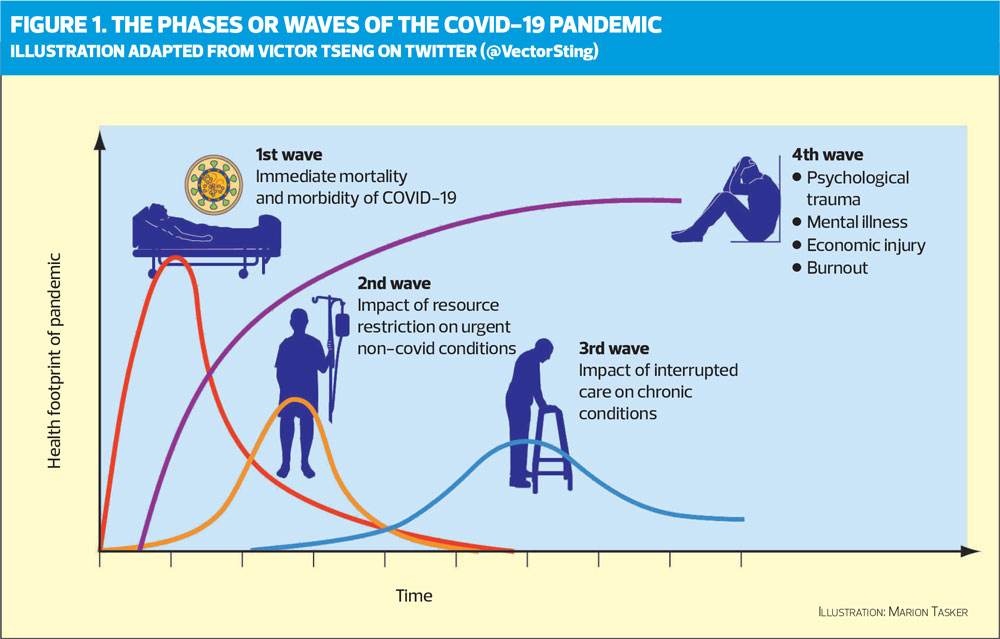
As the current COVID-19 peak passes, general practice is looking to ‘restore’ to the new ‘normal’ (whatever that means!). If the first wave or phase represents the immediate mortality of COVID-19, we are now in transition from the first to second and third phases of the pandemic (Figure 1) – although we need to be acutely aware of a second wave of infections as lockdown restrictions are eased.
Last month (June 2020) the NHS published a Standard Operating Procedure (SOP) for General Practice in the Context of COVID-19.1 The document outlines some of the key principles for general practices, encouraging them to focus on the restoration and second phase of the pandemic. Implementation of these principles will need to be balanced against managing patients who will still present with COVID-19 symptoms, staff wellbeing, a potentially reduced workforce and being mindful of any possible surge or future spike in the virus.
People are using terms such as restoration and recovery though many would agree that we do not want to restore some of the elements and past ways of working. General practice nurses have demonstrated the important and vital role that have played in the managing of the pandemic. Many GPNs have successfully taken on roles that were not necessarily within their current job descriptions such as video consultations and home visits. In addition, patients have demonstrated that they can take control of their own health and this needs to be encouraged.There have been some challenges, but we have seen examples of responsive and effective ways of working that have been innovative and successful. We need to reflect on the successes, sharing across the four nations what has worked well and why. These changes need to be further developed through GPN leadership and utilisations of the wide range of GPNs skills and knowledge for the benefit of the patients within the practice and across the PCN.
The last few months have provided us with a great opportunity to make changes to the way GPNs are currently working and we need to ensure that we are part of the solution in developing future services. This article is based on a strategic document produced by Wessex LMCs to consider how practices deal with the next phase of delivering routine care and coping with the backlog of work while still dealing with the COVID-19 crisis. This is seen as a supportive document for practices, which the LMCs aim to keep up to date. However, the landscape is continually changing, and any future action plans put into place by practices and staff will need to be flexible and responsive.
SO WHAT IS HAPPENING NOW?
Reducing footfall
Practices should by now have well established policies to ensure social distancing is possible, together with infection control measures, including:
- Having individual desk space
- Ensuring surfaces, including desks and chairs, can be cleaned
- Staggering coffee/lunch breaks
- Designated crockery and cutlery for staff
- One-way system for entering and leaving the building
- Appropriate cleaning of doors, handles, toilets, communal areas etc
Clinicians should create socially distant spaces – no hot desking! – and clean their own space including seating, desks, and equipment after each patient and at the end of the day.
As an example of how to reduce staff numbers ‘on site’, one practice has up to one in three of the GPs on any given day working from home, and only one nurse at the practice. One secretary is in the practice, the others work from home. One member of the scanning team is practice-based, the rest are at home. Half the receptionists and members of the practice management team are in the surgery, half at home. IT, healthcare assistants, and phlebotomists remain on the practice premises.
Social distancing with patients
Each clinical activity should be triaged to determine whether it can be managed remotely. If a face-to-face (F2F) appointment is needed, consider where it should take place and who should undertake the activity.
As more services are reintroduced, practices are likely to see an increase in the number of patients seeking an appointment and more patients attending the surgery. This means that measures that were introduced at the start of the pandemic are now even more important. Practices should have set up a one-way entrance and exit system (if possible) and have floor markings to indicated measured 2m spacing distancing, including in clinical areas. The number of patients attending at any one time should be limited. Internal doors should be kept open to reduce contact, and windows should be open where possible to ensure a free flow of air.
Patients should be informed when making their appointment that they should not attend if they have symptoms of COVID-19, and that they will have to wear a mask when they come into the practice. They should be appropriately triaged to hot and cold sites, and will need to be briefed on how to access the building. Ask them to come on their own if possible, and to bring urine samples, for example, with them to avoid having to use toilet facilities at the practice.
On arrival, take the patient’s temperature – although be aware that some people with COVID-19 are asymptomatic and apyrexial. Patients attending the surgery should wear a face mask (some practices are having these provided by volunteers) and remind the patient not to touch surfaces as far as possible. If provided by the practice, masks should be disposed of before leaving the surgery.
ACTIVITIES THAT NEED TO CONTINUE
Most practices have adopted a system of offering specific clinics at cold sites, or specified appointment times. The services that can be delivered depends on the staff and skill mix available, but could be extended by working at primary care network (PCN) level.
- Childhood immunisations – mandatory
- Long term condition reviews
- Shielded patients
- Injections (see Joint injections, below)
- INR (warfarin patients)
- Disease modifying antirheumatic drugs (DMARDs)/Shared care drugs monitoring
- Dressings
- Flu clinics
Allocate longer times for appointments, to allow staff to don and doff PPE – this may mean involving more than one member of staff.
Although the restrictions on shielded patients have been relaxed – they can now leave their home, for example, for daily exercise, and can spend time outdoors with one other person – they should access medical assistance online or by phone wherever possible. They should only attend the surgery for appointments that are absolutely essential.2 If the patient needs F2F assessment they should be seen on a home visit where possibly, ideally by a dedicated team, and not brought into general practice premises unless clinically indicated, and following infection control guidance.1
ACTIVITIES THAT COULD BE RESUMED
Activities that may have been postponed and which could now be resumed dependent on demand and capacity include
- Cervical cytology – See Smears in a time of COVID-19
- Post-natal checks – Offer at cold sites or specific appointment times, and offer 1st baby immunisations at the same time
- Routine adult vaccinations (shingles, pneumococcal)
- Long acting reversible contraception (LARCs) – see Resources: FRSH guidance
- Blood monitoring
Use cold sites for vaccinations, cervical cytology, LARCs, ECGs, dressings, and bloods. Appointments for patients needing dressings should be provided at a cold site, but consider educating the patient – or their carer or a family member – on self-management, if appropriate, or consider using alternative dressings that do not need changing as frequently. If the practice is operating as a hot site, they should negotiate with their PCN to allow their patients to be seen at a different practice.
When resuming LARCs services, make the woman aware of the potential risk of exposure if they wish to attend, or follow FSRH advice on extending use of intrauterine devices or offering an alternative method of contraception (See resources).
Long term conditions
The review of patients with LTCs can often be carried out remotely (See Remote control: the respiratory annul review, page 16, and Diabetes: the annual review in lockdown and beyond, Practice Nurse May 2020;50(5):14-18). Use video consultations – or video group consultations – where possible. Encourage patients to self-record vital signs using digital apps – a range of apps are available from the NHS apps library, and encourage them to use My Health apps designed specifically to help them self-manage the most common long term conditions. There is also a primary care support package from UCL Partners that provides pathways,3 covering:
- The identification of patients with long term conditions
- Stratification of their risk
- Mobilising the wider workforce (healthcare assistants, clinical pharmacists, physician associates) to support the proactive management of patients
- Enabling patient self-management
For patients with COPD (or suspected asthma) see note on spirometry, below.
Managing winter pressures
The flu immunisation programme is likely to be more challenging because of the impact of COVID-19. While at the time of writing, no decision had been taken, NHS England4 says it is in discussions about expanding the flu programme for this autumn, to avoid the potential for a serious flu outbreak coinciding with a possible second wave of coronavirus. Practices have already been asked to ensure that they have ordered sufficient stocks of vaccine for currently eligible patients to meet ‘at least national ambitions and previous uptake rates, whichever is higher’.
‘Flu vaccination is one of the most effective interventions we have to reduce pressure on the health and social care system this winter, and this coming winter we may be faced with co-circulation of COVID-19 and flu… it is more important than ever to make every effort to deliver flu vaccination. Those most at risk from flu are also most vulnerable to COVID-19.’
GPNs are likely to have to deal with both an increase in demand for flu vaccination in all groups this year and also the concerns of some patients in at risk groups about maintaining social distancing when being given the vaccine.
But NHSE is urging practices to attempt to give flu vaccination as soon as vaccine become available, usually from September, and complete vaccination by the end of November where possible.
Non-essential services
Ear irrigation is not considered an essential service in most cases, as long as the patient has been clinically assessed according to the Rotherham care pathway (See Resources). It is also an aerosol generating procedure (AGP) so unless clinically necessary, it should not be undertaken. If considered clinically necessary, adherence to strict PPE and infection control measures is paramount. This is a good time to ensure that your patient information leaflet on ear care self-management is up to date.
Joint injections and minor surgery are not priority services, but if performed, strict PPE and infection control measures should be followed.
Spirometry is not considered an essential service – and is also considered an AGP. Routine respiratory function testing should not currently be performed in primary care, unless part of a coordinated Hub, based around PCNs, with all the appropriate precautions in place.5
Before undertaking any AGP activity, a full risk assessment should be carried out (including staffing, skills, competencies and training) and staff should wear FFP3 masks and full PPE. FFP3 masks need to be expertly fitted, and you should contact your CCG infection control lead for further advice.
WHAT NEEDS TO BE IN PLACE?
The future and success of the ‘restore and recovery’ stages will be a long road and is likely to depend on:
- More joint working across PCNs
- Adopting a collaborative approach with clinical colleagues across health and social care providers and the voluntary sector
- More ‘joint working’ within the wider multidisciplinary teams (MDT) to meet the needs of an increasing number of patients with ill health and complex needs
- Signposting patients to social prescribers and health coaches
- A greater influence on the utilisation of IT, technology, video consultations and triage with reduced face to face patient contact
- A more flexible approach to employment including home working
- Time, support and a dedicated focus on staff mental health and well being
- Increased patient empowerment, education and self-management with the use of Apps such as mymhealth (https://mymhealth.com/file/mymhealth/pdf/mymhealth.pdf) for long term conditions
- Access and effective use of PPE & infection control
- Being creative in how care is delivered to patients with long term conditions (LTCs) e.g. Use of video consultations including group consultations
- Staff and practices being able to respond and react to any surge and spikes
- Engaging staff in the development and delivery of new services and innovation
- Celebrating the important role of GPNs and their impact in primary care
We also need to look at ways of retaining GPNs and encouraging others to see general practice as a great place to work. This will include supporting students within practices ensuring they have a great experience (and will come back) and looking at portfolio careers that could span primary, community and secondary care. The elephant in the room around pay terms and conditions still needs to be addressed especially in line with the new roles across PCNs.
COVID-19 will have affected us all in some way and potentially will have an impact on the mental health and well being of ourselves and colleagues. We will need to focus on being more resilient which is about enabling people to do more because they are better able to manage themselves and those around them.
Trying to think of new ways of working differently, carrying on with the day job and catching up with the backlog can be tiring and at times all-consuming but there is help available. The NHSE Time for Care Project (https://www.england.nhs.uk/gp/gpfv/redesign/gpdp/releasing-time/ ) can provide support to implement new services and innovation. It is free and you can find examples of case studies where things have worked well, for example:
- A drive through children’s vaccine scheme
- Planning the flu campaign for 2020/21
- How to run a virtual planning meeting
Innovation starts with reflecting on the way things are currently, the limitations and restrictions that are in place and using a series of tools and techniques to work out a way of achieving the outcome you want. If innovation were easy, everyone would do it. Ensure the team feel motivated, energised, and confident in their capability to ‘do’ innovation and challenge the way you and others think.
REFERENCES
1. NHS England. Guidance and standard operating procedures: General practice in the context of coronavirus. Version 3.2; 10 June 2020 https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/CO485_guidance-and-standard-operating-procedures-general-practice-covid-19.pdf
2. Public Health England. Guidance on shielding and protecting people who are clinically extremely vulnerable from COVID-19; updated 5 June 2020. https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19
3. UCL Partners Long term condition support. https://uclpartners.com/long-term-condition-support/
4. NHS England and NHS Improvement. National flu immunisation programme 2020/21. https://www.england.nhs.uk/wp-content/uploads/2020/05/national-flu-immunisation-programme-2020-2021.pdf
5. Association for Respiratory Technology & Physiology. ARTP Guidance – Respiratory function testing and sleep services during endemic COVID-19. https://www.artp.org.uk/COVID19

Related articles
View all Articles