Diabetes – putting the patient in control
Beverley Bostock-Cox
Beverley Bostock-Cox
RGN MSc MA QN
Nurse Practitioner Mann Cottage Surgery, Moreton in Marsh
Education Facilitator Devon Training Hub
Primary Care Cardiovascular Society Council Member: pccsuk.org
Practice Nurse 2021;51(4):18-22
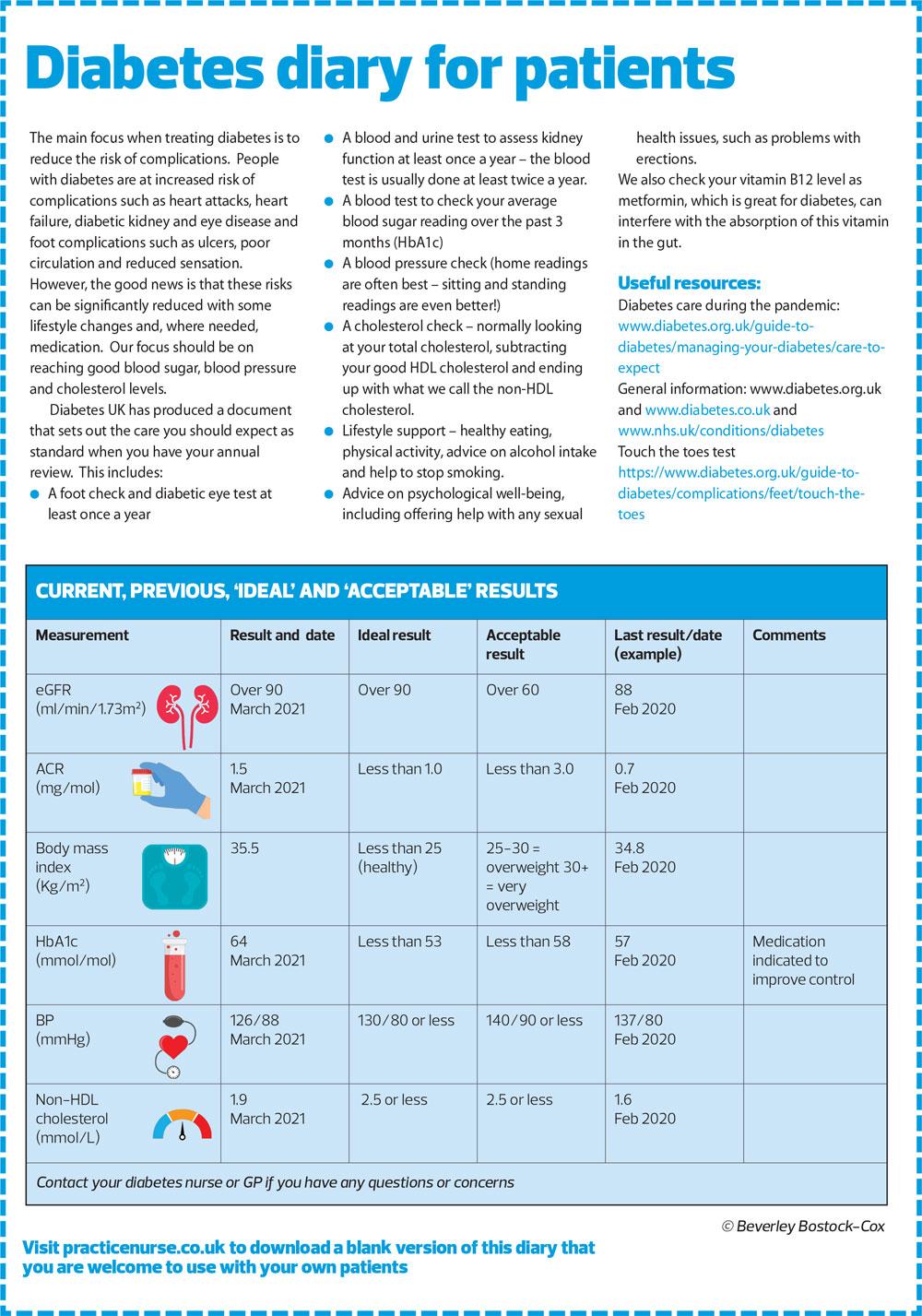
Providing patients with diabetes with a diary can help them take more control of their own health and focus on areas of diabetes management that need closer attention
Over the past year, the switch to remote consultations has necessitated an increase in people monitoring their own health. In diabetes and cardiovascular reviews, for example, patients have been asked if they have access to a home blood pressure machine and could inform the practice of their blood pressure (BP) readings, rather than waiting for readings to be recorded on site in the practice. The guidance issued on reducing cardiovascular disease during the pandemic recommended encouraging people to buy their own home BP monitor if they did not already have one.1 The importance of home BP readings had been highlighted in the National Institute for Health and Care Excellence (NICE) hypertension guidelines, which endorsed the use of home readings for diagnosing and monitoring hypertension.2
This focus on home BP monitoring also meant that patients had the opportunity to ask about ideal values and specific blood pressure targets if they were being treated. All of this led me to consider how much people knew about their measurements – blood results, blood pressure, body mass index and so on – and also how much they understood of the rationale for measuring them. I was specifically interested in how well people living with diabetes understood about how these parameters linked to the risk of diabetes complications.
As a result, I decided to share all of this information with patients by sending them their ‘Diabetes Diary’ via an accuRx message each time they had a review. The feedback has been universally positive, and people have commented on how useful they have found it and how it has helped them to focus on particular areas of their diabetes care. This article explains the content of the diary, along with the rationale for including each area. Readers may like to use this as it stands, or as a template for their own design.
DIABETES AS A CARDIOVASCULAR DISEASE
The incidence and prevalence of type 2 diabetes continues to increase, along with the risk of vascular complications.3 Coronavirus has been linked to a further increase in both type 1 and type 2 diabetes, adding to the future burden on patients and the health service.4 The virus is pro-inflammatory and pro-thrombotic, increasing the risk of diabetes complications, too.4 The risk of diabetes complications, both microvascular and macrovascular, can be reduced through optimised control of blood glucose, lipids and blood pressure5 so people living with diabetes should be aware of their current measurements and how these compare with ideal and acceptable values. In this way they can compare their results with the levels which are linked to a reduced risk of vascular complications and this can support shared decision-making regarding which area to tackle as a priority, and how. Shared decision making is endorsed by NICE.6
RECOGNISING THE LINK BETWEEN DIABETES AND CVD RISK
Diabetes is a cardiovascular disease, with around 80p in every pound spent on diabetes care being spent on addressing the complications of the condition. According to Diabetes UK each week there are 169 amputations, 680 strokes, 530 heart attacks and almost 2000 cases of heart failure due to diabetes and more than 500 people with diabetes die prematurely every week.7
As a result, the focus of diabetes care should be to reduce the risk of complications through appropriate lifestyle and pharmacological interventions.
HOW SHARING THIS LINK MIGHT AFFECT PATIENT BEHAVIOUR
An important element of risk reduction strategies is to ensure that the person living with diabetes understands what we are trying to do and why. The Diabetes Diary aims to explain this while at the same time illustrating for the individual their current results, compared with the ideal values and the acceptable values. Furthermore, previous results can be included so both clinician and the person with diabetes can see the direction of travel. Experience so far indicates that the information is considered to be very useful in informing discussions and decisions. The diary results are sent out via an accuRx message a few days prior to the actual consultation to give each individual time to reflect on them and on any suggestions made by the clinician. It also gives time for people to discuss the results with family, should they want to do so.
CONSIDER HOW MEDICATION FOR DIABETES MIGHT REDUCE RISK
The diary highlights the fact that risk reduction focuses on three key features – glycaemic control, blood pressure control and lipid management. If the individual is not reaching the recommended targets, advice is included regarding how medication (along with lifestyle changes) might help the target to be achieved. The diary offers a starting point for the conversation about these changes. A raised body mass index, for example, might influence discussions about weight loss, and those conversations might include information about local weight loss classes, along with information-sharing about medication which can not only improve glycaemic control but which can also aid weight loss. A QRisk score can be included in the diary for primary prevention, helping the patient to understand their own risk score and how that might help to influence decisions about risk reduction strategies. It is important to point out that many blood glucose lowering therapies come with additional benefits, such as weight loss but also including the fact that they can reduce the risk and impact of cardiovascular disease, heart failure and renal impairment.8 Furthermore, the risk of hypoglycaemia and weight gain with older therapies can be virtually eradicated with newer options.8
HOW CAN ADVICE ON LIFESTYLE INTERVENTIONS IMPROVE PATIENTS’ WELL-BEING?
During the pandemic, there have been some anecdotal reports that people living with diabetes have gained weight, lost their focus on healthy eating and have reduced their level of physical activity. In fact, it could be argued that this doesn’t just apply to people with diabetes! However, during a recent webinar Professor Partha Kar, diabetologist and National Specialty Advisor for Diabetes with NHS England, reported that many of his patients had done the opposite and had invested extra time in improving their health, possibly recognising the increased level of risk that people with diabetes were at, with respect to COVID-19, and the complications from this condition.4
Wherever any individual might sit within this spectrum, the diary offers the basis for discussions about newer dietary interventions, such as a very low calorie diet or a low carbohydrate approach, so the patient knows that there are other options apart from the ones they have tried previously. With regard to physical activity, discussion about preferred types of activity and newer approaches such as interval training might be initiated. Smoking cessation has increased during the pandemic and the diary lends itself to a conversation about whether this is something the patient has achieved, or would like help with, especially if quitting is seen as the ‘new normal’.
The diary can be adapted to each individual in order to reflect key areas of importance for the patient and the clinician to discuss. Providing the diary to people living with diabetes has meant that they now seem to initiate conversations which, in the past, I had to start, sometimes with difficulty. The diary also highlights any missing information. For example, recent research suggested that urine samples for albumin creatinine ratio were not being collected, recorded or acted on.9 By including it in the diary, I am reminded to check for the most recent sample and inform the patient if the check has been missed. I can then not only request a sample, but also explain to the patient why it is so important, with the ACR measurement often deteriorating before the eGFR does.
CONCLUSION
In summary, shared decision making can only be achieved with an informed patient, who has knowledge and understanding of how different aspects such as glycaemic control, blood pressure, lipid management, QRisk score and lifestyle interventions impact on their overall risk of cardiovascular complications. The Diabetes Diary can help to provide a starting point for these conversations and may also encourage the patient to focus on key areas for improvement. The diary should not be used in place of the diabetes review but to inform the diabetes review, for both clinician and patient. It is designed to be short and easy to understand but can also be adapted to each individual – for example including advice on smoking cessation services or the individual’s QRisk score before discussing lipid lowering therapy.
REFERENCES
1. Oxford Academic Health Science Network (ASHSN), Getting It Right First Time (GIRFT) and Primary Care Cardiovascular Society (PCCS); CVD prevention during the COVID-19 pandemic: a guide for primary care https://pccsuk.org/
2020/en/node/newsitem-new-guidance-helps-primary-care-teams-deliver-best-cvd-services-during-the-pandemic
2. NICE NG136. Hypertension in adults: diagnosis and management; 2019 https://www.nice.org.uk/guidance/
ng136
3. Diabetes UK. Diabetes Prevalence; 2020 https://www.diabetes.org.uk/professionals/position-statements-reports/statistics/diabetes-prevalence-2019
4. Bornstein SR, Dalan R, Hopkins D, et al. Endocrine and metabolic link to coronavirus infection. Nat Rev Endocrinol 2020;16:297–298 https://doi.org/10.1038/s41574-020-0353-9
5. Rutter MK, Nesto RW. Blood pressure, lipids and glucose in type 2 diabetes: how low should we go? Re-discovering personalized care. European Heart Journal 2011;32(18):2247–2255 https://doi.org/10.1093/eurheartj/ehr154
6. NICE. Shared decision making; 2021 https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/shared-decision-making
7. Diabetes UK. Diabetes Facts and Stats; 2019 https://www.diabetes.org.uk/resources-s3/2019-02/1362B_Facts%20and%20stats%20Update%20Jan%202019_LOW%20RES_EXTERNAL.pdf
8. Buse JB, Wexler DJ, Tsapas A, et al. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2020;63:221–228 https://doi.org/
10.1007/s00125-019-05039-w
9. Feakins B, Oke J, McFadden E, et al. Trends in kidney function testing in UK primary care since the introduction of the quality and outcomes framework: a retrospective cohort study using CPRD. BMJ Open 2019;9:e028062 https://bmjopen.bmj.com/content/9/6/e028062
Related articles
View all Articles