
COPD guidelines – plus ca change or vive la difference?
Beverley Bostock-Cox
Beverley Bostock-Cox
RGN MSc MA QN
Nurse Practitioner Mann Cottage Surgery, Moreton in Marsh
Education Lead, Education for Health, Warwick
Hard on the heels of the overdue update to NICE guidelines on COPD came a new report from GOLD. So how do the two guidelines compare – and are there lessons to be learned from both?
At the end of 2018, both the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the National Institute for Health and Care Excellence (NICE) updated their guidelines on the diagnosis and management of chronic obstructive lung disease (COPD).1,2 The GOLD committee usually updates its guidance annually but for NICE this was the first update for 8 years. This revamp was well overdue, particularly in the face of new evidence about the management of COPD. In this article, we discuss the similarities and differences between the two guidelines and consider how this influences hands-on practice.
By the end of this article you should be able to:
- Recognise what the two guidelines advise about making the diagnosis of COPD
- Differentiate between COPD phenotypes and how these influence treatment decisions
- Appreciate the different treatment algorithms within each guideline and recognise the rationale for these approaches
- Consider how reversibility in COPD is assessed and managed
- Note the different approaches to managing exacerbating patients and reflect on why each approach might be used
- Be aware of the recommendations about treating COPD holistically
DIAGNOSIS
When it comes to the diagnosis of COPD, the NICE guideline remains largely unchanged from the previous guidelines. NICE states that any patient over 35 with breathlessness or cough should be suspected of having COPD and that the diagnosis will be based on the presence of symptoms and signs, which are supported by objective evidence of abnormal spirometry.2
The advice on spirometry is that it should be quality assured, and that it will normally demonstrate the presence of irreversible airflow obstruction, i.e. an FEV1/(F)VC ratio of less than 70% (0.7) with an FEV1 which is most often (but not exclusively) less than 80% of predicted. The FVC is often normal (>80% predicted).3 NICE also discusses the use of the lower limit of normal (LLN) when interpreting spirometry results.
The GOLD guidelines1 say much the same about the diagnosis of COPD but do not endorse the use of the LLN, stating that there is no evidence for using this parameter to confirm the spirometric patters of irreversible airflow obstruction. Interestingly, the British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) asthma guidelines do recommend the use of the LLN.4 NICE continues to point out that a normal spirometry result may still be compatible with a COPD diagnosis whereas an abnormal result in the absence of symptoms does NOT constitute a diagnosis and GOLD says much the same, pointing out the importance of spirometry while still recognising its limitations. In both guidelines, spirometry is seen as an adjunct to the diagnosis of COPD, not a stand-alone diagnostic tool. There can be no substitute for good history taking to decide on the likelihood of symptoms of breathlessness and cough being due to COPD.
Of note, the place for spirometry at follow up is, according to NICE, is in order to identify a loss in FEV1 of 500 ml or more over 5 years as this may help to identify those who have rapidly progressing disease. As a result of identifying those at risk, referral and investigation may be initiated for these individuals.
CLASSIFYING COPD
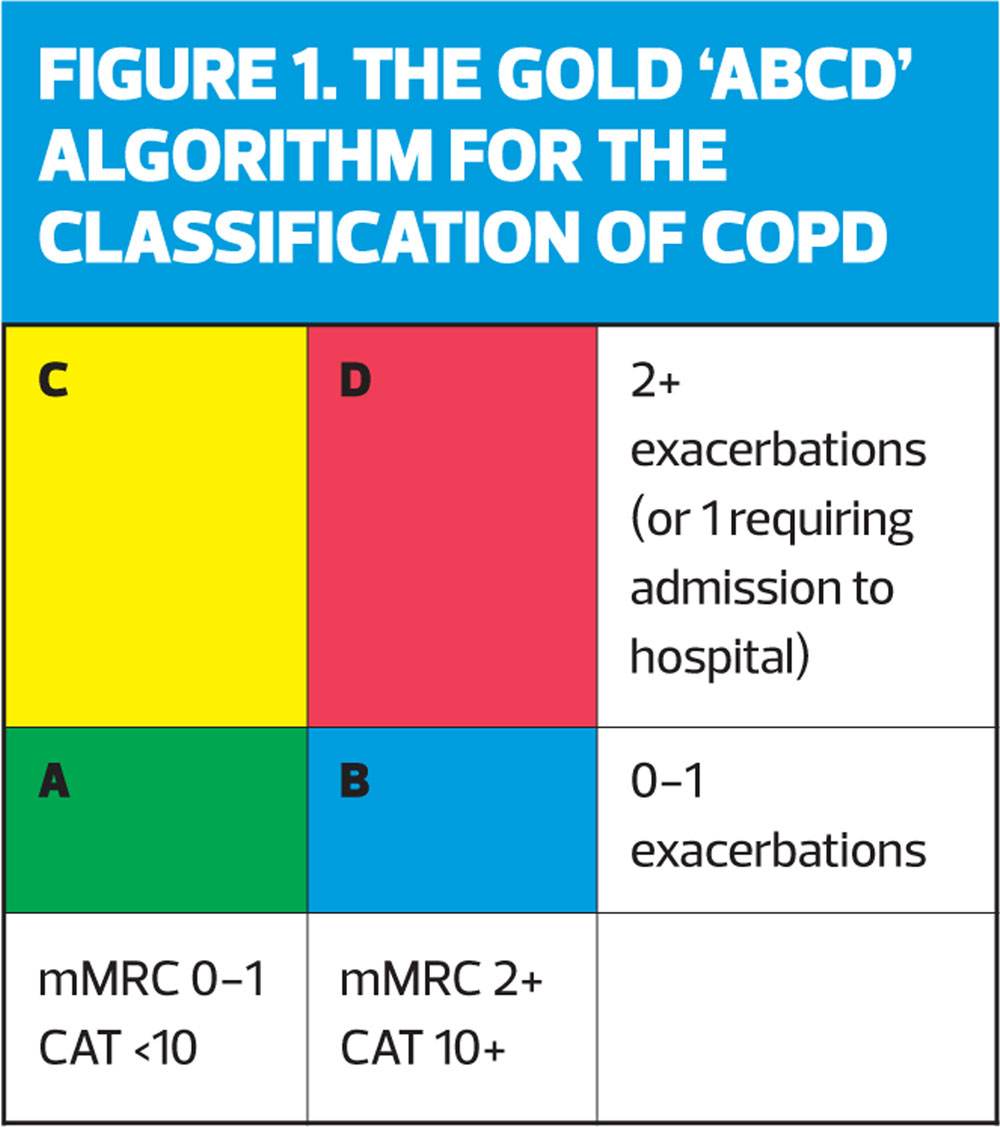
GOLD continues to recommend that people with COPD are categorised using the ABCD algorithm (Figure 1) based on symptom scores such as the modified MRC dyspnoea scale and/or the COPD assessment test and their exacerbation history, which is a recognised predictor of exacerbation risk.5 Unlike GOLD, NICE does not have a clear classification system. Instead, the new NICE guidelines tends to take a ‘one size fits all approach’ to classification and treatment. This is discussed further below.
REVERSIBILITY IN COPD
COPD is often thought of as an irreversible condition where giving a bronchodilator may improve symptoms but will not impact on lung function. However, ‘COPD’ is also an umbrella term that covers a range of conditions such as emphysema, chronic bronchitis, and chronic asthma.6 It is also recognised that smokers with asthma have an increased risk of developing fixed airways disease on top of the underlying asthma component.7 The BTS/SIGN asthma guidelines acknowledge this in their description of reversibility where they state that a change of 12% and 400ml in the FEV1 pre- and post-bronchodilator is clear evidence of reversibility, but that changes of 200ml show that a lower level of reversibility is present.4 The basis of asthma treatment is the use of inhaled corticosteroids, so any asthma element, including evidence of reversibility must, therefore, be recognised when making treatment decisions in people who have asthma with COPD. It is thought that up to one person in five will have a reversible element to their COPD.8 Both the NICE and the GOLD guidelines focus on the importance of establishing any reversible element before deciding on the most appropriate treatment pathway, particularly when it comes to the use of inhaled corticosteroids (ICS).
TREATMENT ALGORITHMS
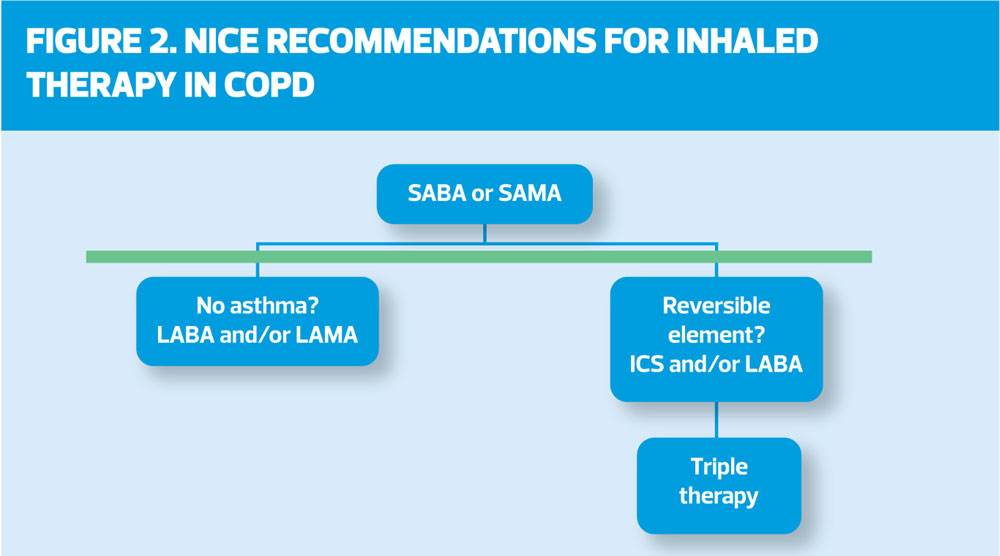
NICE’s recommendations for inhaled therapies in the management of COPD are summarised in Figure 2.
NICE states that anyone with COPD will require a short acting bronchodilator, either a beta2 agonist (SABA) or a muscarinic antagonist (SAMA). As SABAs have a faster onset of action than SAMAs they are more often the drug of choice.9 For those patients who need more treatment – either because they remain breathless or because they are having exacerbations – a dual bronchodilator is recommended, skipping the monotherapy step, which might often be taken, for a more pragmatic approach. There are four dual bronchodilators on the market at present and consideration should be given to the relevant devices as well as the drugs in each product.10
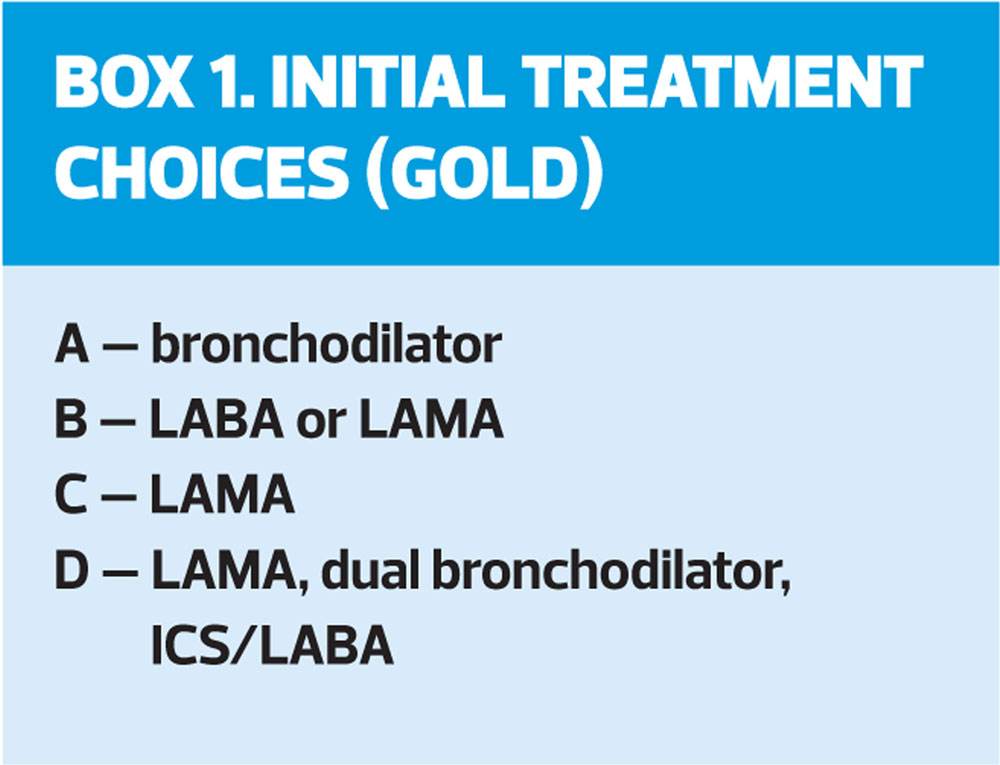
GOLD takes a slightly different approach, although it is not profoundly different. The focus is still on bronchodilation, but there are more nuances to GOLD’s approach. Rather than recommending a dual bronchodilator across the board, GOLD continues to recommend that people with COPD are categorised using the ABCD algorithm (Figure 1) and treated accordingly. So, the first step of treatment for each category, as advised by GOLD, is shown in Box 1.
If an individual does not respond well enough to this initial treatment, GOLD states that there are different factors that will influence which way to go next. These include whether the patient:
- Is predominantly breathless
- Is predominantly exacerbating
- Has raised eosinophils
- Has any evidence of an asthma component to their condition.
In breathless patients, the following recommendations are made:
- Use a long acting beta2 agonist (LABA) or a long acting muscarinic antagonists (LAMA)
- Move up to a dual bronchodilator (LAMA/LABA)
GOLD suggests that although an ICS/LABA or triple therapy might be used in this group, eosinophil levels and exacerbation rates should inform their initiation or ongoing use. Eosinophils over 300 cells/µL suggest potential benefit, as do eosinophils over 100 in the presence of two or more exacerbations in the past year (or one severe enough to require admission). However, NICE goes on to say that in this ‘breathless’ group, ICS therapies should be used with caution especially if there is a history of pneumonia, previous use of an ICS has had no effect or it was inappropriately prescribed in the past. In these situations, de-escalation of therapy away from ICS-based treatments should be considered.
In people who are exacerbating, the following recommendations are made:
- If on bronchodilator monotherapy, move to a dual bronchodilator
- Consider an ICS/LABA if eosinophils are >300 cells/µL or >100 cells/µL with two or more acute exacerbations of COPD (AECOPD)
- In those who are still suffering from AECOPD on either of these, they can be considered for a move up to triple therapy (ICS/LABA/LAMA).
There are two triple therapies on the market at present: Trimbow® (extra-fine beclometasone with formoterol and glycopyrronium) and Trelegy® (fluticasone furoate with vilanterol and umeclidinium).
NICE and GOLD both recommend caution when using inhaled corticosteroids in people with pure COPD i.e. when there is nothing in the history or lung function to suggest that there is any reversible (i.e asthmatic) element to their condition (see NICE section 1.2.9). To that end, and with a nod to both bioethical and medico-legal concerns, NICE recommends that clinicians should be prepared to discuss the risk of side effects (such as pneumonia and diabetes) in people who take inhaled corticosteroids for COPD. This will apply to ICS/LABAs as well as triple therapy. NICE is carrying out a review of the evidence for triple therapy in COPD (ICS/LABA/LAMA therapies) and a further update is anticipated later this year. At the moment NICE recommends that any inhaler with an ICS component should, for the most part, be reserved for people who have asthmatic features which might suggest steroid responsiveness and in those who remain breathless or have exacerbations despite taking an ICS/LABA (section 1.2.14).
PEOPLE WHO CONTINUE TO EXACERBATE
For people who are having four or more exacerbations a year despite treatment as above, prophylactic antibiotics, specifically azithromycin, may be indicated – and this recommendation is mentioned in both guidelines. NICE recommends that these patients should be considered for referral first and foremost, but that if deemed appropriate, ‘pulsed’ azithromycin can be used to prevent further exacerbations, i.e. using a dose of 250 mg 3 times a week. NICE points out that this treatment is most likely to be cost-effective if the patients do not smoke and have optimised both pharmacological and non-pharmacological interventions including inhaled therapies, have had flu and pneumonia vaccinations and (if appropriate) have been referred for pulmonary rehabilitation. If these provisos apply, and the patient continues to have very frequent or prolonged productive exacerbations that may require hospitalisation, the risk: benefit ratio of azithromycin is likely to be in favour of prescribing it. Before prescribing azithromycin, however, sputum culture and sensitivity (including tuberculosis culture) should be carried out, along with training in airway clearance techniques,11 and a CT scan of the chest to rule out other pathologies. The main side effects of azithromycin include hearing loss and cardiac arrhythmias so NICE recommends carrying out an ECG before starting the drug and a hearing test, along with liver function tests. It goes without saying that these side effects should be explained to the patient before commencing treatment in order to comply with medico-legal principles such as the Montgomery ruling.12 Azithromycin use should be reviewed after 3 months and at least twice yearly after that. It should be noted that at this stage, using azithromycin in this way would constitute off licence prescribing. GOLD also endorses the use of azithromycin in this situation, but points out that at this time, there is only evidence of potential benefit for up to one year.
RESCUE PACKS
GOLD and NICE both say that rescue packs, consisting of antibiotics and oral steroids, may be useful for people who have an AECOPD. In December 2018, NICE published its guidance on the use of antibiotics in people with AECOPD, which recommend a cautious approach to the use of antimicrobials.13 Furthermore, steroid doses differ between the two guidelines. In line with the REDUCE study,14 GOLD recommends a dose of 40mg for 5 days, whereas NICE is sticking with its 14-year-old recommendation to use 30mg for 7-14 days. However, this recommendation will be included in a further review of oral steroids in acute exacerbations, which is due to be published in June 2019.
HOLISTIC TREATMENT
NICE recommends that before starting any inhaled therapy, smoking cessation support should be offered, along with advice about having both the flu and pneumonia vaccines. Pulmonary rehabilitation referrals should also be offered where resources are available. In people who are made anxious by breathlessness, a referral for cognitive behavioural therapy should be considered, if available. Both guidelines point out the importance of recognising the role of co-morbidities in people with COPD that might affect symptoms – for example, a new presentation of cor pulmonale may initially be mistaken as an acute exacerbation of COPD. Co-morbid conditions such as arthritis may influence mobility and lead to further deconditioning, and low mood may impact on someone’s ability to engage with lifestyle changes and take regular treatment. In essence, clinicians are reminded to take their COPD blinkers off, as these patients are at risk of a range of conditions, often as a result of a long smoking history.
CONCLUSION
In summary, both the NICE and the GOLD guidelines point out the importance of making the correct diagnosis, basing this on the history, symptoms and risk factors and backed up with spirometry. While the NICE guidelines recognise that people with COPD may have different symptoms patterns, GOLD provides a specific tool for assessing the optimal approach to management, using symptoms and exacerbation scores to inform the ABCD algorithm. NICE’s approach to treatment is a pragmatic one where it recognises the benefits from early treatment with dual bronchodilators and the importance of using inhaled corticosteroids with care. GOLD takes a more ‘stepped’ approach to treatment and includes long acting bronchodilators as monotherapy as well as using them as dual bronchodilators. GOLD takes a similar view of inhaled corticosteroids to NICE, saying that their main role should be in the management of people with a reversible element to their COPD. However, GOLD says that triple therapy may be used in people with COPD who are being treated with a dual bronchodilator if they continue to exacerbate. GOLD has highlighted the potential role of eosinophil levels in predicting which patients may get the best risk: benefit ratio from using an inhaled corticosteroid for their COPD. Both guidelines endorse the use of pulsed azithromycin in people who continue to exacerbate. Although the use of rescue packs is also covered in both guidelines, there are discrepancies over the dose of oral steroids. These may be ironed out when NICE publishes further guidance later this year – at the moment the two guidelines disagree on the appropriate dose and duration of steroid treatment in AECOPD. Both guidelines support the concept of treating people with COPD holistically, recognising the influence that co-morbid conditions, both physical and psychological, might have on COPD management and outcomes. For the general practice nurse seeing people with COPD, suspected or confirmed, it is reassuring to know that in many of the key areas, diagnosis, holistic management and the use of inhaled therapies, NICE and GOLD agree more than they differ. Any persisting differences reflect the ongoing challenges with studies that show contrasting outcomes based on the same therapeutic interventions and underline the need for further research in these areas.
REFERENCES
1. GOLD. 2019 Global Strategy for Prevention, Diagnosis and Management of COPD, 2018 https://goldcopd.org/gold-reports/
2. NICE NG115. Chronic obstructive pulmonary disease in over 16s: diagnosis and management, 2018 https://www.nice.org.uk/guidance/ng115
3. Primary Care Commissioning. Quality Assured Diagnostic Spirometry, 2013 https://www.pcc-cic.org.uk/article/quality-assured-diagnostic-spirometry
4. British Thoracic Society/Scottish Intercollegiate Guidelines Network. Asthma guidelines, 2016. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign- asthma-guideline-2016/
5. Halpin DM, Decramer M, Celli B, et al. Exacerbation frequency and course of COPD. Int J Chron Obstruct Pulm Dis 2012;7:653-61.
6. World Health Organization (2019) Chronic obstructive pulmonary disease, 2019. https://www.who.int/respiratory/copd/en/
7. Sears MR. Smoking, asthma, chronic airflow obstruction and COPD Eur Respir J 2015;45:586-588; DOI: 10.1183/09031936.00231414
8. Soriano JB, Davis KJ, Coleman B, et al. The proportional Venn diagram of obstructive lung disease: two approximations from the United States and the United Kingdom. Chest 2003;124:474-481
9. Ejiofor S, Turner AM. Pharmacotherapies for COPD. Clin Med Insights Circ Repir Pulm Med 2013;7, 17-34. doi:10.4137/CCRPM.S7211
10. Bostock-Cox B. Finding the right combination: choosing combination inhalers for asthma and COPD. Practice Nurse 2017;47(6):18-22
11. Bostock-Cox B. The role of positive expiratory pressure and inspiratory muscle training devices in primary care. Practice Nurse 2015;45(01):12–16
12. Montgomery v Lanarkshire Health Board, 2015. UKSC 11 https://www.supremecourt.uk/decided-cases/docs/UKSC_2013_0136_Judgment.pdf
13. NICE NG114. Chronic obstructive pulmonary disease (acute exacerbation): antimicrobial prescribing, 2018 https://www.nice.org.uk/guidance/ng114
14. Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs Conventional Glucocorticoid Therapy in Acute Exacerbations of Chronic Obstructive Pulmonary Disease: The REDUCE Randomized Clinical Trial. JAMA 2013;309(21):2223-2231
Related articles
View all Articles