Primary care essentials: Stroke prevention
Margaret Perry
Margaret Perry RGN BSc(Hons) MSC
Advanced Nurse Practitioner, Linkway Medical Practice, West Bromwich
Prevention of stroke has become an important part of clinical practice and is an area where practice nurses can and do play a vital role
A stroke has a devastating effect on the patient's health and quality of life and can affect both young and older adults. The condition has a huge impact on hospital beds and services, estimated to cost the economy approximately eight billion pounds per year1 with sufferers occupying around 20% of all acute hospital beds and a further 25% of beds in long term facilities. Not only is the effect on the individual huge but stroke also impacts on friends and family especially when the condition leaves the affected person in need of long term care.
TYPES OF STROKE
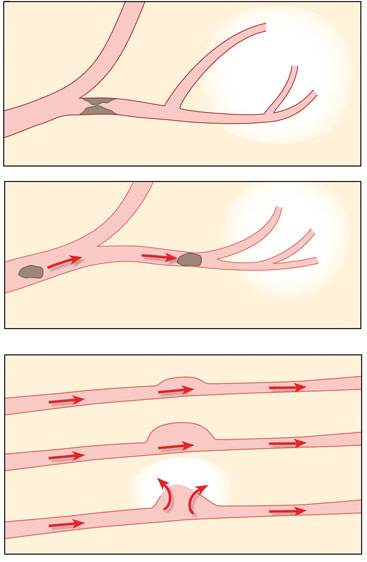
There are essentially two types of stroke, haemorrhagic and ischaemic (Figure 1). The first occurs as a result of a burst vessel leading to bleeding into the brain tissues. The latter occurs as a result of a blockage of the arteries. As different parts of the brain control different function, the effects obviously depend on the area affected and the extent of the damage. Ischaemic strokes are by far the most common accounting for 85-90% of all strokes.2
IMPACT OF STROKE
Current statistics indicate that stroke is the third commonest cause of death in England and Wales, behind heart disease and cancer3 and it is estimated that there are 87,700 first strokes per year in England and Wales and a further 53,700 recurrent strokes.4 Because of the way in which stroke affects the body, the condition carries the risk of long term effects, and it is thought that at least 450,000 people are left severely disabled as a result of stroke in England alone.5 In common with other conditions the risk of stroke increases as we age, although sadly approximately 25% of strokes occur in those below the age of 65.6
GOVERNMENT INITIATIVES
The recent Government FAST campaign, (Box 1) has done much to raise public awareness of the recognition of the signs of the onset of stroke and the need to act quickly in calling for emergency services, and while this has resulted in faster action for stroke sufferers, better still is the prevention of events through lifestyle interventions and treatment of associated risk factors, which is where practice nurses have the opportunity to play a major part.
All practice nurses are now familiar with the Quality and Outcomes Framework of the General Medical Services contract, which offers financial incentives to practices that can provide evidence of blood pressure measurement, cholesterol levels, and smoking status. The whole primary health care team has a role to play in meeting the QOF targets, delivering health promotion and encouraging healthy lifestyles.
NON-MODIFIABLE RISK FACTORS
Non-modifiable risk factors are those that cannot be altered by individual or medical intervention (Box 2). However, while they cannot be modified, knowledge of their influence on stroke risk can enable clinicians to make sure these patients are offered aggressive treatment of any risk factors they may have which can be modified.
MODIFIABLE RISK FACTORS
These are the areas where practice nurses have an excellent opportunity to impact on stroke risk. Many are linked, which means to say that aggressively targeting one area can potentially impact on another. An example of this is perhaps obesity and hypertension, where weight loss may help lower the blood pressure. Practice nurse involvement potentially spans a whole range of interventions from promoting healthy lifestyle, through concordance with medication and for nurse prescribers, prescribing and monitoring treatment for management of hypertension and hyperlipidaemia and diabetes. Table 1 provides a summary of medications useful in stroke prevention.
Each risk factor will be discussed individually, identifying links between them where they exist.
Obesity
The prevalence of obesity is rising in many countries of the world and has become a public health issue because of its link with a number of conditions, including diabetes, cardiovascular disease and certain cancers. Statistics suggest that the numbers of obese people is continuing to rise steadily, with obvious concern for the impact this will have on medical services and health care organisations. Body mass index (calculated from the weight in kilograms divided by the square of the height in metres) has widely been regarded as a useful tool for assessing the level of obesity. However, abdominal obesity determined by the waist to hip ratio is now thought to be an important measurement. The Northern Manhattan Stroke Study6 identified abdominal obesity as a strong and independent risk factor for ischaemic stroke, and more worryingly although relevant to both young and older subjects, the influence of waist hip ratio on stroke risk appeared greater among those under the age of 65 years.
Diet
Poor diet leads to obesity, which can affect blood pressure, and diets high in fat impact on cholesterol levels, both of which are known to increase stroke risk. The impact of poor diet over a number of years also increases the risk of cardiovascular disease and type 2 diabetes: its effects therefore span several chronic diseases leading to both high economic costs and a heavy burden on health services. Current guidance supports a low fat, low salt, high fibre diet rich in fruit and vegetables. Fruit and vegetables contain phytochemicals and antioxidants, which are essential to maintaining health.
During normal body processes, free radicals are produced that have the potential to cause cancer and cell damage. Antioxidants bind to free radicals, converting them to non-toxic compounds, while phytochemicals can prevent replication of cancer cells, help to prevent cell damage and also lower cholesterol levels. Specific phytochemicals are found in different coloured fruit and vegetables whilst the highest concentration of antioxidants is found in fruit and vegetables that are brightly coloured. Studies have shown that eating at least five portions of fruit and vegetables daily reduces the risk of ischaemic stroke by as much as thirty per cent.7
Hyperlipidaemia
The link between hyperlipidaemia and stroke risk has been more difficult to clarify, but a number of studies have indicated that hyperlipidaemia may be an independent risk factor for ischaemic stroke.8 Statins are the mainstay of medical treatment for hyperlipidaemia, but it is important for patients to play their part by improving their diet and making lifestyle changes alongside their treatment.
Hypertension
High blood pressure is the single most important risk factor for stroke, increasing the risk of both ischaemic and haemorrhagic strokes. It is suspected that many people have hypertension for some time before it is diagnosed, increasing the damage done while the condition remains untreated. Untreated hypertension damages blood vessels and organs, and causes enlargement of the heart as it pumps harder to keep the blood circulating. The benefits of treating hypertension have long been recognised and a study of treatment trials throughout the world, reviewing nearly 50,000 patients found a 38% reduction in all strokes, the effects of which applied to both blacks and whites.9 When assessing blood pressure, it is well worth checking the pulse at the same time: atrial fibrillation is a major treatable cause of stroke. It is thought to be a factor in almost half of all ischaemic strokes and the cause of one-in-four strokes in those over the age of 80.10
Alcohol intake
Levels of alcohol consumption in the UK are a cause for concern because of the increasing prevalence of alcohol-related illnesses, the impact on individual and public health and, of course, the added pressure on health services. The effects of alcohol on stroke risk have been extensively studied with some inconsistency in the findings. While light to moderate consumption is thought to provide some protective benefit, with a reduced stroke risk, heavy alcohol consumption is associated with an increased risk of both haemorrhagic and ischaemic stroke. The way in which excessive alcohol intake affects stroke risk is believed to involve various mechanisms, including alcohol-induced hypertension, cardiomyopathy, coagulation disorders, atrial fibrillation and reduction in cerebral blood flow.11
Exercise
The association between physical activity and stroke risk has been under scrutiny with conflicting results: some studies have found no effect of exercise on stroke risk, some have found some beneficial effect, but some studies actually suggest increased risk, particularly with high impact exercise. The theory is that sudden intense exercise may cause an unstable atherosclerotic plaque to dislodge, leading to a thrombotic event. However, regular moderate levels of exercise are encouraged because of their role in weight loss, improving insulin sensitivity and decreasing blood pressure, and both the American Heart Association/American College of Cardiology Guidelines for Primary Prevention of Cardiovascular Disease and Stroke,12 and the European Stroke Initiative Recommendations for Stroke Management13 include physical activity as one of the most important primary prevention measures for stroke risk reduction.
Smoking
Involvement in smoking cessation has been an important part of the practice nurse workload for a long time, and will continue to be, given the ever-present concerns relating to the health effects of long term smoking. As well as its association with chronic obstructive pulmonary disease, lung cancer and peripheral vascular disease to name but a few, cigarette smoking approximately doubles a person's risk of stroke.14
Red flags
Signs and symptoms that warrant urgent attention are shown in Box 3
MOTIVATING BEHAVIOURAL CHANGE
Educating and advising patients is a key part of the practice nurse role but motivating behavioural change can be notoriously difficult. Helping the patient to understand the effect of behaviour on their health is imperative. For change to occur, they must believe that their behaviour makes them vulnerable to a particular health problem, that the problem is potentially serious, and that the benefits of taking action outweigh the potential costs.15 Setting small achievable goals with changes that can be incorporated into daily life has proved helpful, such as using the stairs instead of the lift, and walking to the local shops instead of using the car can be become the norm. Where the change required is more difficult to achieve, such as smoking cessation or losing a significant amount of weight, referral to other agencies may be needed. Organisations which may be helpful are suggested in Table 2.
CONCLUSION
Stroke and its impact on patients, their families, and of course the cost of care and the impact on health services is clearly of concern. By focusing on those at risk, practice nurses have the opportunity to make a real difference - and indeed, many will be doing so already. Because of the number of risk factors involved, practice nurses have the opportunity for professional development, increasing their knowledge across a range of areas, which will benefit all their patients and will hopefully help to reduce the number of patients affected by stroke in the years to come.
REFERENCES
1. Pearson TA, Blair SN, Daniels SR et al. American Heart Association Guidelines for Primary Prevention of Cardiovascular Disease and Stroke. Update. Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. Circulation 2002; 106: 388-91.
2. Hack W, Kaste M, Bogousslavsky J et al. European Stroke Initiative Recommendations for Stroke Management- update 2003. Cerebrovasc Dis 2003; 16: 311-37.
3. Wolfe, C "The Burden of Stroke" in Wolfe, C, Rudd, T and Beech, R (eds) Stroke Services and Research (1996) The Stroke Association
4. Office of National Statistics. Stroke Incidence and Risk Factors in a Population-based Cohort Study. Office of National Statistics Health Statistics Quarterly 2001;12 (Winter 2001)
5. Department of Health. Reducing Brain Damage: Faster access to better stroke care, National Audit Office Report. London; Department of Health: 2005
6. Suk SH, Sacco RL, Boden-Albala B, et al. Abdominal Obesity and Risk of Ischemic Stroke: The Northern Manhattan Stroke Study. Stroke 2003;34:1586-1592
7. Colorado Department of Public health and environment (2012) 5 a day and chronic disease.
http://www.cdphe.state.co.us/pp/COPAN/5-a-day/5ADAYChronicDiseases.html
8. Reynolds K, Lewis LB, Nolan JD, et al. Alcohol Consumption and Risk of Stroke: A Meta-analysis. JAMA 2003;289(5):579-588
9. Roger VL, Go AS, Lloyd Jones DM et al. Heart Disease and Stroke Statistics 2011 Update: A Report From the American Heart Association. Circulation 2011; 123: e18-e209
10. Mayo Foundation for Medical Education and Research (MFMER) (2010) Stroke. http://www.mayoclinic.com/health/stroke/DS00150/DSECTION=causes
11. Howard G, Anderson R, Sorlie P, et al. Ethnic differences in stroke mortality between non-Hispanic whites, Hispanic whites, and blacks: the National Longitudinal Mortality Study. Stroke1994;25:2120-2125.[
12. Gorelick P, Sacco R, Smith D, et al. (1999) Prevention of a first stroke: a review of guidelines and a multidisciplinary consensus statement from the National Stroke Association. JAMA. 281:1112-1120
13. Gorelick PB, Schneck M, Berglund LF, et al. Status of lipids as a risk factor for stroke. Neuroepidemiology. 1997; 16:107-115.
14. Elder JP, Ayala GX, Harris S. Theories and Intervention approaches to health-behavior change in primary care. Am J Prev Med 1999;17:275-284.
15. MacMahon S, Rodgers A. The epidemiological association between blood pressure and stroke: implications for primary and secondary prevention. Hypertension Research 1994;17(suppl 1):S23-S32.
19. Eftimovska N, Stojceva-Taneva O, Polenakovic M. Slow progression of chronic kidney disease and what it is associated with. (2008) US National Library of Medicine, National Institutes of Health. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18709007
Related articles
View all Articles