Prostate Cancer – where are we now?
Dr Ed Warren
Dr Ed Warren
FRCGP, FAcadMEd
November is the month when there is a particular focus on men’s health, in a bid to tackle the ongoing discrepancies between men and women’s health outcomes and life expectancy: one of this year’s target areas is prostate cancer
According to Wikipedia, ‘Movember’ was invented by some blokes in a pub in Adelaide, Australia, in 1999.1 During November men grow a moustache to raise money for charity. Apparently ‘mo’ is an Australian abbreviation for moustache and so Movember is a mash-up. By 2004 another and unrelated group in Melbourne were using the same approach to raise awareness of prostate cancer and depression in men, and so started the Movember Foundation charity. The idea spread through Australia and then to Europe and America, and by 2011 the charity had raised $174m worldwide.1 The current emphasis is on prostate cancer, testicular cancer, and suicide in men.
So why have a focus on men’s health? The reality is that men do relatively badly compared to women in the health stakes as well as having a liability to some diseases (such as prostate cancer) which women just don’t get. The Men’s Health Forum publishes statistics on men’s health in the UK.2 Life expectancy for males in the UK in 2014 was 78.2 years compared with 82.3 years for women. Within this span, men can expect to be healthy for 63.5 years, and women for 65.7 years. There is a considerable variation with social class, so that men in the most deprived 10% of society can expect to die at 74.1 years, whereas those in the least deprived 10% will on average be drawing their pensions up to age 83.1 years. In the UK nearly one man in five (19%) dies before getting to the age of 65. The main killers in men are cancer and circulatory disorders (stroke and heart attack). Men have a 14% greater chance than women of getting cancer, and a 37% greater risk of dying from cancer.2
But why is it that men die young, or at least younger than women? The Men’s Health Forum offers the following reasons,2 reasons which suggest there is room for improvement:
- Men have on average lower levels of health literacy than women. They know fewer facts about health. They don’t read prescription inserts, and they are more likely to buy prescription drugs on the internet.
- Men are less likely than women to visit a GP or a pharmacy. The pharmacy figures are particularly stark: on average men visit the pharmacy four times a year whereas women visit 18 times. Men delay seeking help for a number of cancers and are less likely to engage with bowel cancer screening.
- A facade of masculinity may lead to symptoms being played down (‘it’s just old age’); to stoicism and a need for control (not wanting to involve third parties such as the NHS); and an increase in risky behaviours such a smoking and heavy drinking.
PROSTATE CANCER
The prostate is a wedge-shaped gland found only in males (and also in people born male, such as trans-women). It is made mainly of smooth muscle, and is situated at the base of the bladder, surrounding the urethra. The normal prostate is about 20g (roughly the size of a golf ball) and grows with age from about 35 years onwards, so that at age 85 virtually all men will have evidence of enlargement.3
Urinary symptoms in men are very common. Lower Urinary Tract Symptoms (LUTS) include urinary frequency, nocturia, urinary dribbling and incontinence. Roughly a third of men over the age of 50 will have moderate to severe LUTS. Looking at nocturia as a single symptom, between 30% and 60% of men over age 70 will be troubled.4 ‘Nocturia’ here is defined as getting up to pee twice or more times each night – nocturia less than this, i.e. once a night, is unlikely to cause much inconvenience or be associated with disease.5
Prostate enlargement can cause urinary symptoms, but in most cases enlargement is due not to cancer but to benign prostatic hypertrophy (BPH). However, much of the preliminary work in primary care for men with urinary symptoms is to rule out cancer.
Prostate cancer is the most common type of cancer in men – about 26% of all new cases of cancer in men are prostate cancer.6 In the UK in 2014, 46,690 men were diagnosed with prostate cancer, so that the lifetime risk of prostate cancer is one in eight. Each year 11,500 men die of prostate cancer.7 Prostate cancer is predominantly a disease of older men (aged 65–79 years) but around 25% of cases occur in men younger than 65.6 You are more likely to contract prostate cancer if you are:
- Over 50 – increasing age is the most important risk factor. Prostate cancer mainly affects men aged over 50 years.
– Autopsy studies show that by the age of 80 years, 80% of men will have evidence of prostate cancer.
- Of black ethnicity – men of black ethnicity are at highest risk of developing prostate cancer
– The lifetime risk of being diagnosed with prostate cancer is 1 in 4 for black men, compared to 1 in 8 for white men.
– Black men are also twice as likely to die of the disease.
- Someone with a family history of prostate cancer – genetics and a positive family history of prostate cancer are associated with increased risk.
– The lifetime risk of developing prostate cancer increases depending on the number of relatives affected and the age at which they were diagnosed.
– About 9% of men have true hereditary prostate cancer – three or more affected relatives or at least two relatives who have developed early-onset prostate cancer (aged less than 55 years).
- Overweight or obese – obesity and being overweight are associated with advanced prostate cancer. Lower testosterone levels increase the risk of more aggressive tumours.
– Men have a 15–20% increased risk of dying from prostate cancer with every 5 kg/m2 increase in BMI.
ROLE OF THE GENERAL PRACTICE NURSE (GPN)
There are a lot of older men out there with LUTS. Nearly all of them will have BPH. Some of them will have prostate cancer, which in a minority of cases will cause their death. A lot more will be worried that they have prostate cancer. How does a GPN become involved?
Some men may present their symptoms during a consultation for something unrelated, often at a chronic disease management clinic (men with LUTS are of an age when they are increasingly likely to have something else wrong with them as well). An appropriate response is required.
Those GPNs who are involved in practice triage may get new cases presenting, or perhaps men who have had a recent worsening of their previously tolerated symptoms, or perhaps who have been talking to someone and decided that something needs to be done.
Ironically, things such as Movember raise the profile of men’s health issues, and perhaps make men more aware of what is normal, what is not normal, and what may be something serious. That is exactly what Movember is designed to do, but the knock-on is that more men will be beating a path to your door.
Some things in the investigation of prostate cancer have changed, and men will want information. Some things in the treatment of prostate cancer have changed. These are mainly secondary care issues, but you need to be able to field any questions.
The issues surrounding Prostate Specific Antigen (PSA) are still hotly debated, particularly whether or not to use the test as a screening procedure.
Male genitalia are a source of some derision (and not just among women). When Doncaster West PCT produced a glossary of Yorkshire medical terms, they identified 21 different words for male genitals9 as though men in Yorkshire would do anything to avoid talking about them properly. Men are reluctant to admit to problems ‘down below’, so may be so embarrassed that the information has to be teased out with some care and consideration. Less than half of men with LUTS will seek help.10 Although GPNs are renowned for their tact and discretion, and so are in a perfect position to find out what is going on, some men may be reluctant to discuss these issues with the predominantly female GPN workforce.
GATHER THE EVIDENCE
Anyone with a prostate who has LUTS should be suspected of having prostate cancer until proven otherwise. You might also want to gather information about risk factors for prostate cancer (in particular a family history). Other symptoms which suggest prostate cancer may occur with or without LUTS, and can usefully be explored. Ask about any unexplained symptoms of:
- Lower back, or bone pain. Prostate cancer, together with lung, thyroid, kidney and breast, are the five cancers that typically spread to bone
- Lethargy
- Erectile dysfunction
- Haematuria
- Anorexia/weight loss.
‘Unexplained’ here means that your patient is not known to have another and unrelated condition which might be causing the symptoms. For example a building worker with 20 years of low back pain which has not got appreciably worse or altered in character will not fall into the ‘unexplained’ category.
By this stage you will be advising your patient to see one of your GPs. Further tests and investigations will be required, and very probably a referral to hospital will be needed.
Some patients will not want to take things any further. They may just want reassurance, and indeed the majority of men with LUTS do not have prostate cancer. Even if prostate cancer is present, it may not cause any problems. In the UK in 2012-2014:12
- 94% of men survived prostate cancer for at least one year
- 85% of men survived prostate cancer for five years or more
- 84% of men survived prostate cancer for 10 years or more.
But finding out which prostate cancers are likely to be, or become, aggressive depends on a more thorough assessment.
‘WHAT WILL HAPPEN WHEN I SEE THE GP?’
Other patients may ask you what a trip to the GP will entail. After talking through the symptoms, two offers will be made. One is to do a blood test for PSA (and also possibly for other things such as kidney function – obstructed urine outflow leads to backpressure and possible kidney damage). The other is the Digital Rectal Examination (DRE). NICE uses the word ‘offers’ referring to PSA and DRE, and it has to be your patient’s informed choice, but the offers will be accompanied by a deal of pressure to comply, and any reluctance may well be met with grizzly stories about the possible health penalty for declining.
The pros and cons of DRE
DRE is recommended as the rectal route is the only way of clinically examining a prostate gland. Most prostate cancers start in the outer layers of the gland and so can, in theory, be felt by an experienced clinician. However, the commonest prostate cancers are less than 2mm across, and these are unlikely to be felt on DRE.13 A DRE provides further information, but it is far from a foolproof definite way of diagnosing or excluding prostate cancer.
The pros and cons of PSA
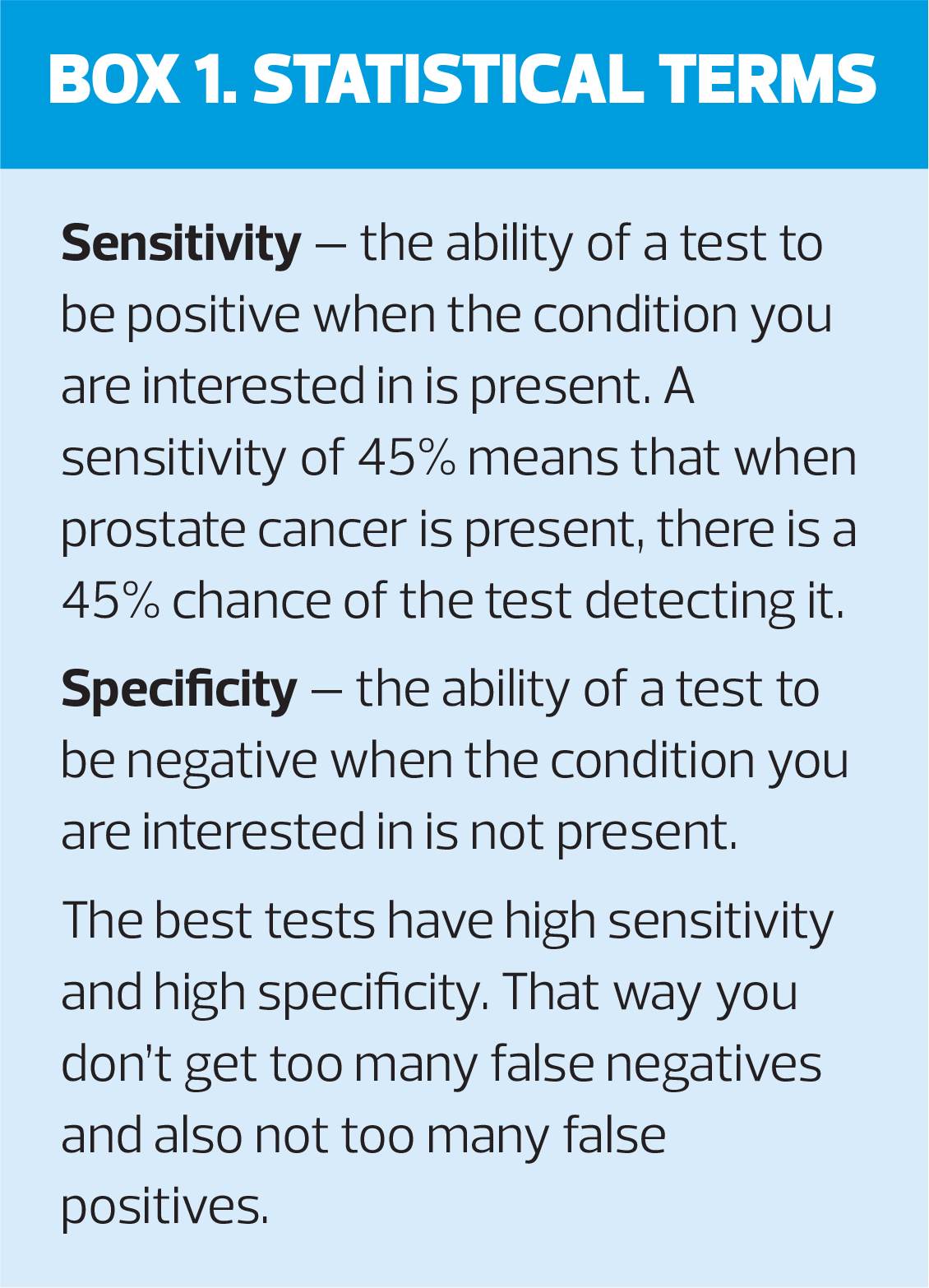
PSA is a protein made in the prostate. It liquefies semen to make it flow better, and also possibly helps spermatozoa to penetrate into ova. It is present in high concentration in semen, and in even higher concentrations if prostate cancer is present. Some of it leaks out into the blood where it can be measured. Available since 1986, PSA was not the first blood test for prostate cancer. Prostatic Acid Phosphatase testing has been available since the 1940s and was previously the blood test of choice, but it is made by things other than prostates and so has a sensitivity for prostate cancer of only about 45% (that is, slightly less accurate than tossing a coin).14 PSA is a lot better than this – PSA plus DRE has a sensitivity for prostate cancer of 96%,15 but a poor specificity (Box 1).16
How does this translate to patients in the real world? NICE recommends a number of decision aids and information sources for men who are thinking of whether to have the test.17 In summary, the figures are:17
- False negatives: 15% of men with a negative PSA test will in fact have prostate cancer. Of these 2% have a high-grade cancer.
- False positives: 75% of men with a positive PSA test will not have prostate cancer. This results in unnecessary investigations such as prostate biopsy and unnecessary treatments.
‘WHAT WILL HAPPEN IF I GO TO HOSPITAL?’
The men referred to hospital will have suspected cancer, and so are referred under the relevant cancer protocols, the ‘2 week wait’ system. Indeed, NHS England has also produced guidance for secondary care detailing an even more rapid service, leading to prostate cancer being investigated and diagnosed or excluded within 14 days of a GP referral.18 For a patient more accustomed to waiting an age to see a consultant in outpatients, this may be alarming. Referrals are made electronically, appointments are booked urgently with phone calls, and all hell is let loose. Things must truly be serious – except that they are not: current guidance on urgent suspected cancer referrals suggests a 3% threshold – for all patients referred under these protocols only 3% will turn out to have cancer and 97% will not.19
A referral for possible prostate cancer will almost always result in an offer of a prostatic biopsy, guided by Trans Rectal UltraSound (TRUS) – a TRUS biopsy. Ten or twelve small tissue samples are taken from the gland using a rectal approach. Depending on the microscopic images obtained, the presence of cancer is confirmed (but only 45% of cancers are detected at biopsy20), and the Gleason Score is assessed – this score estimates the likely aggressiveness of the cancer based on the microscopic appearance of the cancer cells.
The results of the PROMIS study have changed all this.21 This was a multi-centre study in the UK on 740 men referred for possible prostate cancer from 2012 to 2015, and published in 2017. It sought to establish whether the initial use of multi-parametric magnetic resonance imaging (mpMRI, a specialised type of MRI) would improve diagnostic accuracy and prevent unnecessary TRUS biopsies. And it does. The use of mpMRI reduces the need for TRUS biopsy by 25%, diagnoses 90% of clinically relevant prostate cancer (the ones likely to cause harm), and shows fewer cancers which are less significant (the ones unlikely to cause harm). Since TRUS biopsy is deeply unpleasant, and can cause bleeding and infections, this is a win-win situation, except that the necessary equipment is expensive.
NICE has acknowledged this emerging truth,20 and majority of UK citizens now have access to mpMRI. However, there are stark regional variations: according to 2018 figures for England, London and the south east have the best coverage, but mpMRI to PROMIS standards is less widely available in the north east and north west.22 Scotland has five scanners, Wales two and Northern Ireland none at all which meets the PROMIS standards.
If cancer is confirmed, there are several treatment options. The one recommended will depend on the staging of the cancer (how big it is and how far it has spread), the PSA level and the Gleason score. In three broad categories:23
- Do nothing or ‘watchful waiting’ with repeated PSA testing. Many prostate cancers found are unlikely to interfere with life or cause premature death, so just keep an eye on things. A variant of this is ‘active surveillance’ where regular PSAs are supplemented with one mpMRI and repeated DRE and TRUS biopsy.
- Prostate destruction through surgery (which can now be done laparoscopically, assisted by robot), through radiotherapy, or through brachytherapy where small radioactive seeds are planted in the prostate.
- Adjunctive or palliative treatment with chemotherapy, bisphosphonates, strontium or hormones – for example, goserelin (Zoladex) implants.
Just how much patient preference informs the treatment offered is not clear from the guidance. Different management strategies are ‘indicated’ for different situations. Generally, watchful waiting and active surveillance would seem appropriate only for low risk prostate cancers, and prostate destruction treatments for the more potentially troublesome ones. But some men will not like the thought of a wait-and-see approach, and would prefer their prostate cancer to be removed and out of harm’s way. For others the side effects of prostate surgery will be more than they can contemplate – the risks of the surgery itself, erection problems, infertility, incontinence.
Conclusion
Men die younger than women, and one important reason for this is that they get prostate cancer. However, prostate cancer is nothing like as common as LUTS, but LUTS is the major reason why a prostate cancer diagnosis is considered. PSA was supposed to change all that, but has in fact added to the complications because of the false positives and false negatives it produces.
For those who end up in hospital with prostate cancer, many can be just left alone. For the rest surgical and radiotherapy techniques are improving all the time and many men survive without trouble for years with their hormone implants.
The use of PSA as a screening tool has not been covered. The Americans want to screen and the British – using exactly the same evidence base – do not. We will discuss the use and abuse of PSA as a screening test in men with no symptoms in the next issue of this journal.
REFERENCES
1. Wikipedia. Movember https://en.wikipedia.org/wiki/Movember
2. Men’s Health Forum. Statistics. https://www.menshealthforum.org.uk/statistics
3. Muir G. Benign prostatic disease. General Practitioner February 13 1998:58-60
4. Rees J, Bultitude M, Challacombe B. The management of lower urinary tract symptoms in men. BMJ 2014;348:25-28.
5. Tikkinen KA, Johnson TM, Tammela TL, et al. Nocturia frequency, bother, and quality of life: how often is too often? A population-based study in Finland. Eur Urol 2010;57(3):488-96. doi: 10.1016/j.eururo.2009.03.080
6. NICE CKS. Prostate cancer – prevalence. https://cks.nice.org.uk/prostate-cancer#!backgroundSub:2
7. Prostate Cancer UK. https://prostatecanceruk.org/prostate-information/about-prostate-cancer
8. NICE CKS. Prostate cancer – What are the risk factors for prostate cancer? https://cks.nice.org.uk/prostate-cancer#!backgroundSub:3
9. Doncaster West PCT. Glossary of Yorkshire Medical Terms. https://regmedia.co.uk/2006/04/24/glossary_for_international_recruits.pdf
10. Hunter DJW, McKee C M, Black NA, et al. Health care sought and received by men with urinary symptoms and their views on prostatectomy. Br J Gen Pract 1995;45:27-30.
11. NICE CKS. Prostate cancer. What are the signs and symptoms of prostate cancer? https://cks.nice.org.uk/prostate-cancer#!diagnosisSub:1
12. NICE CKS. Prostate cancer – what is the prognosis? https://cks.nice.org.uk/prostate-cancer#!backgroundSub:4
13. Scroder FH. Prostate cancer: to screen or not to screen? BMJ 1993;306:407-8.
14. Stamey TA, Yang N, Hay AR, et al: Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N Engl J Med 1987;317:909-916
15. Payne S. Current management of prostatic problems. Update 1996;52:184-92
16. Muir G. Prostate cancer. General Practitioner May 1 1998:60-62.
17. NICE CKS. Prostate cancer. Information about PSA testing. https://cks.nice.org.uk/prostate-cancer#!diagnosisAdditional:3
18. NHS England. Implementing a timed prostate cancer pathway. April 2018 https://prostatecanceruk.org/media/2496723/nhs-england-implementing-a-timed-prostate-cancer-diagnostic-pathway.pdf
19. NICE NG12. Suspected cancer: recognition and referral. https://www.nice.org.uk/guidance/ng12/chapter/Introduction
20. NICE CKS. Prostate cancer. What investigations may be performed in secondary care? https://cks.nice.org.uk/prostate-cancer#!diagnosisSub:5
21. Ahmed HU, Bosaily AE-S, Brown LC, et al, for the PROMIS study group. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet 2017; 389: 815–22
22. mpMRI: Standards and availability in the UK. https://www.google.com/maps/d/viewer?mid=1a732RFPeoTWJTwF0mGhAAcb_GFz4RGCp&ll=55.5185784454211%2C-2.786392949999936&z=5
23. NICE CKS. Prostate cancer. Scenario: management. https://cks.nice.org.uk/prostate-cancer#!scenarioRecommendation:3
Related articles
View all Articles