|
July 2024 The why and how of foot assessments in diabetes Foot checks in people with diabetes were one of the casualties of the COVID-19 pandemic, and performance rates have still not returned to pre-pandemic levels. But they are essential if preventable amputations are to be avoidedWHY FOOT ASSESSMENTS IN DIABETES?A Diabetes UK survey in 2017 showed that 1 in 3 people with diabetes did not know that foot ulcers are a serious complication of their condition. Foot ulcers can lead to foot and leg amputations, and to early death. Amputations relating to diabetes are increasing in young and middle-aged adults in the UK.1 An annual foot check is one of the nine core care processes for someone with diabetes and is often performed by general practice nurses. During the pandemic, many of the care processes for people with diabetes were missed. The greatest impacts of the pandemic were on foot examination, weight measurement, and retinal screening.2 Performance of these core processes remains lower than pre-pandemic levels. Foot checks are vital to ensure patients are aware of their current foot risk score, which is an indicator of the probability of a serious foot problem. In England, 7,957 major (above the ankle), 21,738 minor (below the ankle) diabetes related amputations and 171,759 foot-disease-related hospital admissions were reported for the period 2017/18 to 2019/20.3 Every 20 seconds a limb is lost somewhere in the world.4 Managing the diabetic foot, coupled with the cost of associated lower limb amputations, costs the NHS in England up to £1 billion annually.5 Up to 80% of diabetes-related amputations, with a 50% five-year mortality, are avoidable.6 The increase in volume and associated value of clinical negligence claims involving patients with diabetes-related lower limb complications is increasing and led to a report and recommendations by NHS Resolution in 2022.7 Foot assessments identify the presence of risk factors for foot complications in diabetes, which could lead to foot ulceration, infection and amputation. The foot assessment should determine the patient’s risk of foot problems so that the patient can be advised of their risk status and provided with relevant education for self-management and, most importantly, when to seek urgent advice. FREQUENCY OF ASSESSMENTSThe NICE guideline on the prevention and management of diabetic foot problems [NG19] recommends that children with diabetes who are under 12 years, and their family members or carers (as appropriate), should be given basic foot care advice.8 For young people with diabetes who are 12 to 17 years, the paediatric care team or the transitional care team should assess the young person's feet as part of their annual assessment and provide information about foot care. If a diabetic foot problem is found or suspected, the paediatric care team or the transitional care team should refer the young person to an appropriate specialist. For adults with diabetes, assess their risk of developing a diabetic foot problem:
HOW TO UNDERTAKE A FOOT CHECK1. Take a historyRecord the patient’s medical, surgical and social history. Record information about their foot care. Ask
Record if the patient is unable to self-care, or suffers from any of the disabilities listed below, as this can increase the risk of foot problems.
2. Perform the examinationPerform a visual inspection of both feet including heels, soles and in between the toes checking for signs of swelling, inflammation, skin colour, callus, blisters, fissures (cracks in hard skin) ulceration, deformity, nail problems, signs of infection. Perform a vascular assessment of both feet. Palpate pulses in the feet or use a handheld doppler ultrasound which may be more reliable than palpation alone.
If pulses are absent the patient may require an in-depth vascular assessment to determine if there are problems with blood flow to the feet. If the patient complains of cramp in the calf when walking any distance (claudication), which is relieved by rest, this may also be a sign of peripheral arterial disease. Perform a sensory assessment. Diabetes can cause nerve damage causing peripheral neuropathy. There may be a loss of pain sensation, loss of the awareness of hot and cold, and loss of sensation (sensory neuropathy). These sensations are normally protective mechanisms, which are alerts to tissue damage. With loss of these sensations, tissue damage, ulceration and infection can occur without the patient noticing. Despite neuropathy causing a loss of sensation, some patients have neuropathic pain with symptoms of shooting pain, numbness, burning sensations, and/or pins and needles.
Failure to feel the monofilament at any point indicates a loss of sensation and neuropathy. Neuropathy may also cause change to foot shape such as clawing toes (motor neuropathy) and dry, cracked skin due to loss of sweating (autonomic neuropathy). These should also be considered when testing for neuropathic changes. If a 10g monofilament is not available, the ‘Touch the Toes Test’ can be performed. This test is also known as the Ipswich Touch Test, which was designed by Gerry Rayman and the team at Ipswich Hospital.9
3. Risk stratificationIt is important that the patient knows their foot risk stratification. This will direct how often the patient requires foot review and the type of education they require to prevent foot problems. Risk is assessed as low risk, moderate risk, high risk and active foot problem e.g. ulceration (Table 1). Make sure your patient knows and understands their foot risk score. 4. Provide educationTell your patient their risk score and ensure they know what this means. If they are moderate or high risk, they must be referred to their Foot Protection Service, usually provided by community podiatry services. Patient advice to prevent foot problems for low risk feet10
Further information about footcare in diabetes is available from the Royal College of Podiatry website – see Resources. TIME IS TISSUE!The national diabetes footcare audit has shown that the quicker a person with diabetes and a foot condition sees an expert the better the outcome. The longer patients wait to see a specialist, the more damage can occur to the tissues of the foot. Find out who your local Foot Protection (often community podiatry) and Multidisciplinary Footcare Teams (usually based in hospital) are and advise patients how to contact them if they have a foot problem. There are cards available in different skin tones from Insights for Diabetes Excellence, Access and Learning (iDEAL) called ‘ACT NOW’, (Figure 1) which indicate when a patient should seek urgent attention. REFERENCES1. NHS Digital Report 1: Care Processes and Treatment Targets 2020-21 Full Report; 2022. https://digital.nhs.uk/data-and-information/publications/statistical/national-diabetes-audit/core-report-1-2020-21# 2. National Cardiovascular Intelligence Network. National Diabetes Foot Care Report: 2022. 3. D-Foot International. Foot Facts; 2024 4. National Diabetes Foot Care Audit Fourth Annual Report; 2019 https://files.digital.nhs.uk/FC/18ED7F/NDFA%204AR%20-%20Main%20Report%20v1.1.pdf 5. van Acker K. Diabetic Foot Disease: When the alarm to action is missing. International Diabetes Federation; 2015. https://www.diabetesresearchclinicalpractice.com/article/S0168-8227(15)00325-3/abstract 6. N Mottolini. Diabetes and lower limb complications. A thematic review of clinical negligence claims. NHS Resolution; 2022. https://resolution.nhs.uk/wp-content/uploads/2022/06/Diabetes_and_Lower_Limb_Complications.pdf 7. NIHR. Simple tool identifies the people with diabetes most likely to develop foot ulcers; 2022. https://evidence.nihr.ac.uk/alert/simple-tool-predicts-foot-ulcers-in-diabetes/ 8. NICE [NG19]. Diabetic foot problems: prevention and management; Updated 2019 . https://www.nice.org.uk/guidance/ng19 9. Curtis L, Miller R. The 10-point training tool for staff education in inpatients diabetes. Journal of Diabetes Nursing; 2018. https://diabetesonthenet.com/journal-diabetes-nursing/10-point-training-tool-staff-education-inpatient-diabetes/ 10. Diabetes UK. Testing for sensitivity in your feet. https://www.diabetes.org.uk/guide-to-diabetes/complications/feet/touch-the-toes 11. Royal College of Podiatry. Low risk of non-healing wounds and amputation. https://rcpod.org.uk/patient-information/diabetes/diabetes-leaflets/low-risk-of-non-healing-wounds-and-amputation |
Richard Leigh DPodM, BSc, MRCPod, FRCPodM, FFPM RCPS (Glasg) Consultant Podiatrist, Royal Free London NHS Foundation Trust Council Member, The Royal College of Podiatry Chair, English Diabetes Footcare Network Member of the London Clinical Senate Council Visiting Professor Perm State Medical University Practice Nurse 2024;54(4):16-19 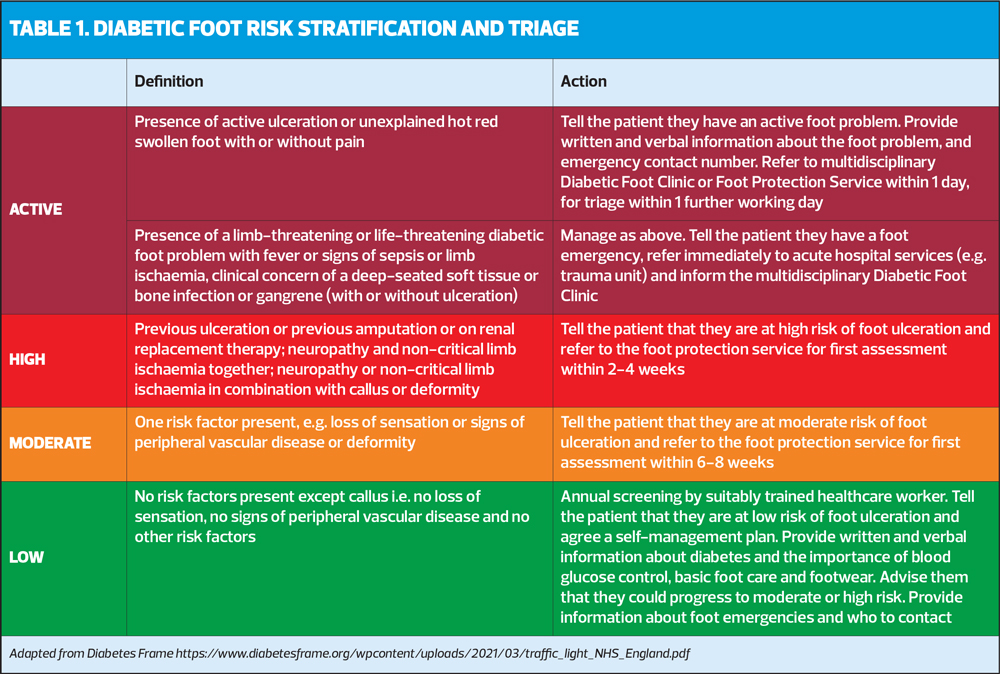 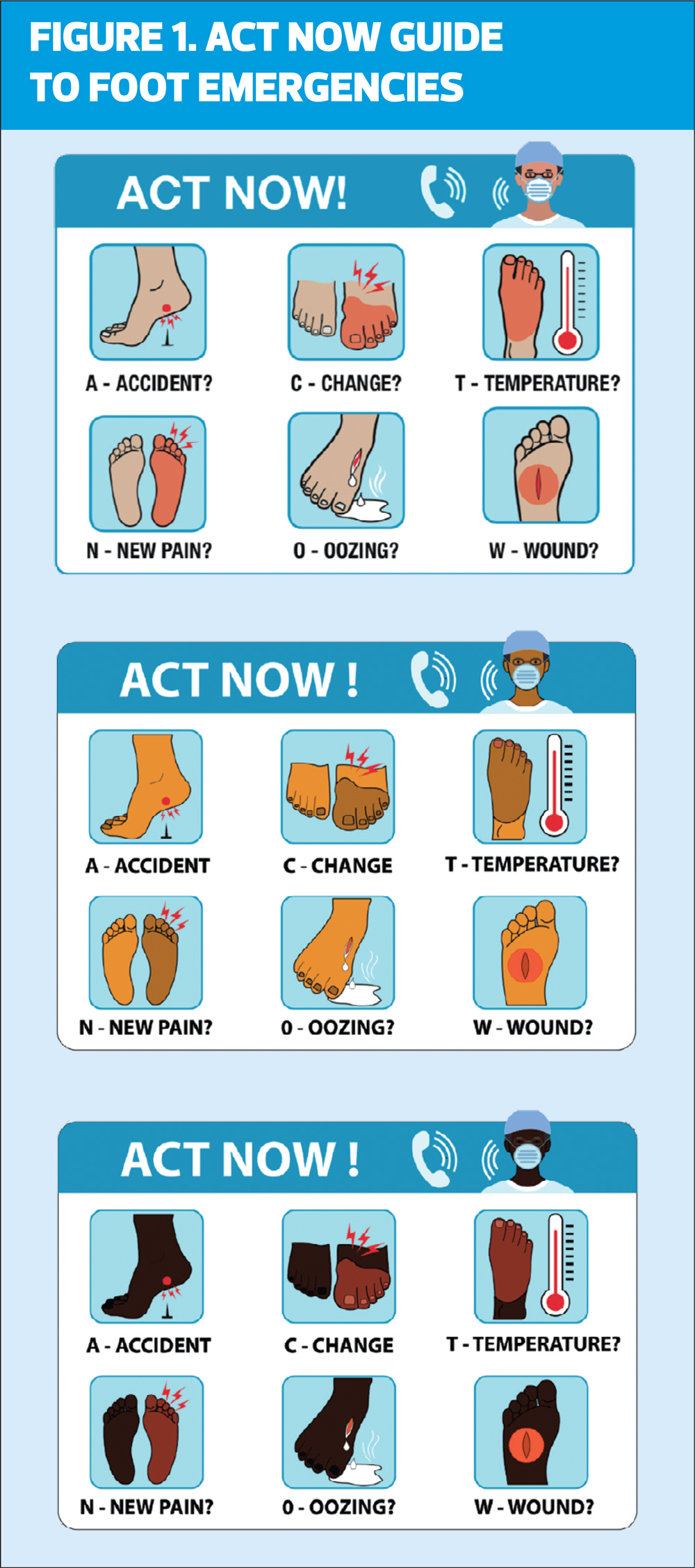  |
Back to top