Chronic obstructive pulmonary disease in over 16s: diagnosis and management
NICE NG115, December 2018
NICE NG115, December 2018
New evidence has emerged and practice has changed in a number of areas since 2010, when the last version of the guideline was published. This evidence and the changes in how care is delivered may have a significant impact on people with COPD
Approximately 1.2 million people have a diagnosis of chronic obstructive pulmonary disease (COPD) in the UK, according to the British Lung Foundation.1 Although there are 115,000 new diagnoses per year, most people with COPD are not diagnosed until they are in their fifties or older and many more people may remain undiagnosed. The UK has the 12th highest recorded deaths from COPD in the world, with an age-standardised mortality rate of 210.7 deaths per million people between 2001 and 2010.
New evidence has emerged and practice has changed in a number of areas since 2014, when the last version of the guideline was updated.2 This evidence and the changes in how care is delivered may have a significant impact on people with COPD, for example by increasing the focus on:
- Treating tobacco dependence
- Optimising inhaled therapy treatments
- Improving access to lung volume reduction procedures
- Predicting and preventing COPD exacerbations.
The costs of some inhaled therapies have also reduced, because they are now off patent and generic versions are available. However, the range and complexity of the inhaled therapies available (drugs and devices) has also increased.
The 2018 guideline2 includes new recommendations on:
- Incidental findings on chest X-rays or CT scans
- Prognosis
- Inhaled therapies
- Prophylactic antibiotics
- Self-management and exacerbation plans
- Oxygen therapies
- Managing pulmonary hypertension and cor pulmonale
- Lung reduction procedures
DIAGNOSIS
The recommendations on diagnosis of COPD remain largely unchanged from the 2004 and 2010 versions, but advice on when to perform spirometry has been updated to include monitoring disease progression.
For people with an incidental finding of emphysema or signs of chronic airways disease on a chest X-ray or CT scan, NICE recommends primary care respiratory review and spirometry – but also reminds clinicians to be aware that the presence of emphysema on a CT scan is an independent risk factor for lung cancer.
If the person is not a current smoker, their spirometry is normal and they have no symptoms or signs of respiratory disease:
- Ask them if they have a personal or family history of lung or liver disease and consider alternative diagnoses, such as alpha-1 antitrypsin deficiency
- Reassure them that their emphysema or chronic airways disease is unlikely to get worse
- Advise them to return if they develop respiratory symptoms
At the time of initial diagnostic evaluation, in addition to spirometry all patients should have a chest X-ray to exclude other pathologies, a full blood count to identify anaemia or polycythaemia, and BMI calculated. Additional investigations should be considered as needed (Table 1).
Initial investigations in suspected COPD | |
Investigation | Role |
Sputum culture | To identify organisms if sputum is persistently present and purulent |
Serial home peak flow measurements | To exclude asthma if diagnostic doubt remains |
ECG and serum natriuretic peptides | To assess cardiac status if cardiac disease or pulmonary hypertension are suspected because of:
|
CT scan of the thorax |
|
Transfer factor for carbon monoxide (TLCO) |
|
COPD or asthma?
Untreated COPD and asthma are frequently distinguishable on the basis of history (and examination) in people presenting for the first time. The following features (unchanged from 2004) can help to make the diagnosis (Table 2).
Distinguishing features in asthma and COPD | ||
COPD | Asthma | |
Smoker or ex-smoker | Nearly all | Possibly |
Symptoms under age 35 | Rare | Often |
Chronic productive cough | Common | Uncommon |
Breathlessness | Persistent and progressive | Variable |
Night-time waking with breathlessness and/or wheeze | Uncommon | Common |
Significant diurnal or day-to-day variability of symptoms | Uncommon | Common |
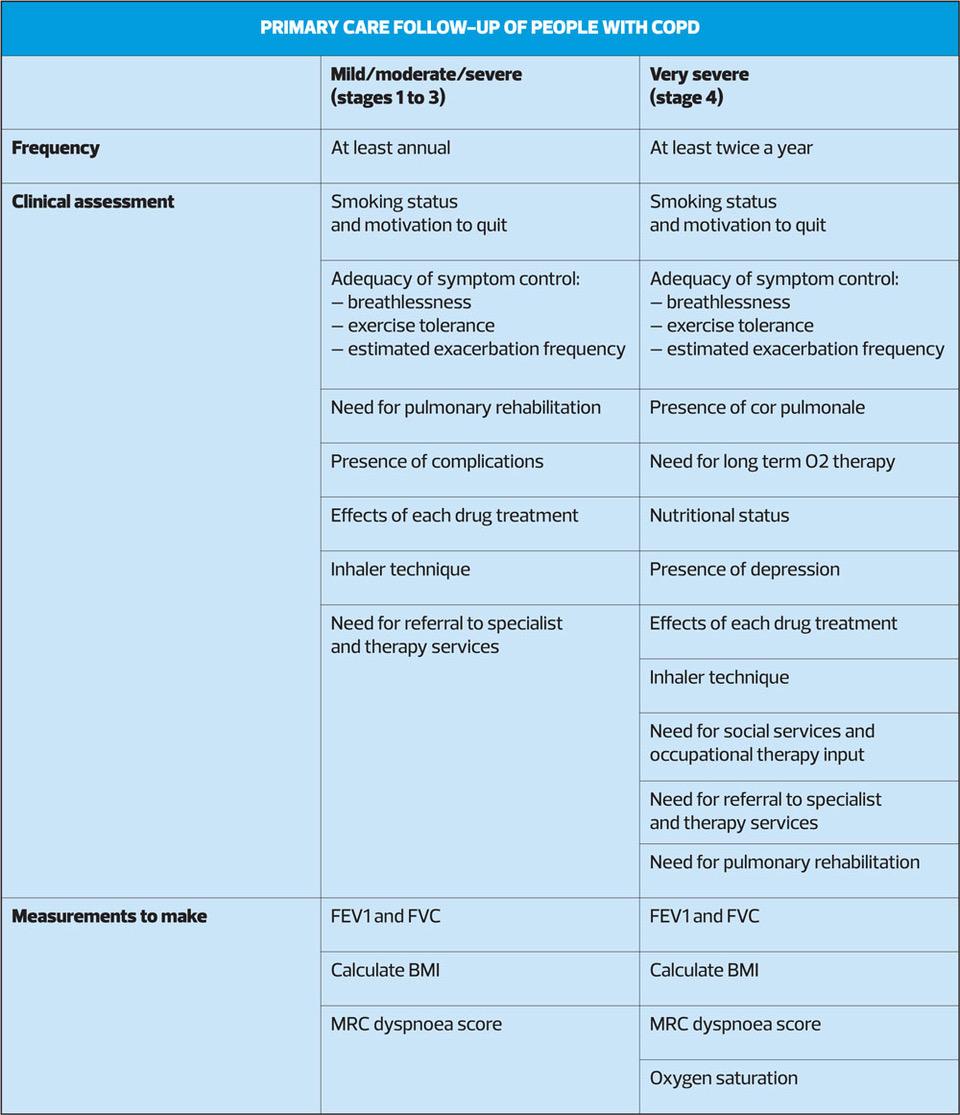
ASSESSING SEVERITY AND USING PROGNOSTIC FACTORS
No single measure can adequately assess disease severity in an individual patient. Use of a multidimensional index (such as BODE) to assess prognosis in people with stable COPD is not recommended, because such tools are unable to classify people reliably into high- and low-risk groups better than FEV1 alone, are no better at predicting outcomes than FEV1 alone, and are time consuming to administer and include components that are not routinely available in primary care.
Instead, from diagnosis onwards, consider:
- FEV1
- Smoking status
- Breathlessness (MRC scale)
- Chronic hypoxia and/or cor pulmonale
- Low BMU
- Severity and frequency of exacerbations
- Hospital admissions
- Symptom burden (e.g. COPD assessment test [CAT] score)
- Exercise capacity (e.g. 6-minute walk test)
- TLCO
- Whether the patient meets the criteria for long-term oxygen therapy and/or home non-invasive ventilation
- Multimorbidity
- Frailty
EDUCATION
At diagnosis and at each review appointment, offer people with COPD and their family members written information about their condition, tailored to the person’s needs, and opportunities for discussion with a healthcare professional who has experience in caring for people with COPD.
As a minimum, the information should include:
- What COPD is and its symptoms
- Advice on quitting smoking (if relevant) and avoiding passive smoking, and how this will help
- Managing breathlessness
- Physical activity and pulmonary rehabilitation
- Medicines, including inhaler technique and the importance of adherence
- Vaccinations
- Identifying and managing exacerbations
- Support organisation
- How COPD will affect other long term conditions that are common in people with COPD, such as hypertension, heart disease, anxiety, depression and musculoskeletal problems.
Give advice on the factors that increase the risk of exacerbations, including:
- Continued smoking or relapse for ex-smokers
- Exposure to passive smoke
- Viral or bacterial infection
- Indoor and outdoor air pollution
- Lack of physical activity
- Seasonal variation (winter and spring)
Patients with COPD should be given an individualised self-management and exacerbation action plan, developed with the individual patient, and this should be reviewed at future review appointments.
When providing exacerbation rescue packs (short course of oral corticosteroids and short course of antibiotics) to keep at home, ensure that the patient knows to tell you when they have used them and to ask for replacements. If they use 3 or more courses in a year, the reasons should be investigated.
MANAGING STABLE COPD
While advice on smoking cessation remains unchanged, NICE has made a sweeping change to its recommendations on inhaled therapy in stable COPD. (For the management of patients with multimorbidity, see the NICE guideline on this topic.3)
Inhaled therapy
As before, the first treatment step for newly diagnosed patients is a short acting bronchodilator (SABA) as initial empirical treatment to relieve breathlessness and exercise limitation.
For most patients who require additional therapy to improve symptoms, the choice should be a combination of long-acting muscarinic antagonists (LAMA) and long acting beta2 agonists (LABA).
This is because the evidence showed that, compared with other dual therapy combinations and with monotherapy, the combination of LAMA+LABA:
- Provides the greatest benefit to overall quality of life
- Is better than other inhaled treatments for many individual outcomes (such as reducing the risk of moderate to severe exacerbations)
- Is the most cost-effective option.
NICE did not recommend a particular LAMA because the guideline development committee was not convinced that the evidence showed any meaningful differences in effectiveness between the drugs in this class. Instead, they updated the existing recommendation on drug and inhaler choice, based on their experience of what factors should be taken into account.
NICE says offer LAMA+LABA to people who:
- Have spirometrically confirmed COPD and
- Do not have features of asthma or features suggesting responsiveness to steroids and
- Remain breathless or have exacerbations despite having been prescribed or offered treatment to help them stop smoking, optimised non-pharmacological management and relevant vaccinations, and using a SABA.
The criteria for offering LABA+ICS are the same, with the exception of:
- Have features of asthma or features suggesting responsiveness to steroids.
Most of the trials specifically excluded people with COPD and asthma, so there was no direct evidence for this group. The committee recommended LABA+ICS (inhaled corticosteroids) based on their clinical experience and knowledge of the likely benefit of ICSs in certain specific COPD phenotypes.
Although the combination therapies recommended in this guideline are the most effective options, some people are currently using different therapies, such as LAMA or LABA monotherapy, and may have their symptoms under control with these. The committee did not want to make people change treatments unnecessarily, so they made a recommendation highlighting that people did not need to switch treatments until their clinical needs changed.
The evidence on triple therapy (LAMA+LABA+ICS) is being reviewed and will inform a further update to the guideline, due to be published in June 2019, but triple therapy can be offered to patients with features of asthma or features suggesting responsiveness to steroids, who remain breathless or have exacerbations despite taking LABA+ICS.
When prescribing ICS for patients with COPD, clinicians should be aware of their potential to cause side effects, including pneumonia.
For patients who are currently being prescribed LAMA or LABA as monotherapy, there is no need to change their regimen unless it is considered clinically appropriate (and the patient is in agreement).
The choice of drugs and inhalers should be based on how much they improve symptoms, the patient’s preferences and ability to use the inhaler(s), the drug’s potential to reduce exacerbations, their side effects and their cost. NICE recommends minimising the number and types of inhalers prescribed as far as possible to it easier for people to use their inhalers correctly. Most people with COPD can acquire adequate inhaler technique with appropriate training – inhalers should only be prescribed after people have been trained to use them and can demonstrate satisfactory technique. Ability to use their inhaler should be regularly assessed, and corrected if necessary. For patients who need to use a spacer, advise them not to clean the spacer more than once a month because more frequent cleaning can lead to a build-up of static and can affect performance. Spacers should be handwashed using warm water and washing up liquid, and allowed to air dry.
The recommendations for when a nebuliser should be used remain unchanged from the previous version of the guideline.
PROPHYLACTIC ANTIBIOTICS
The evidence shows that prophylactic antibiotics reduce the risk and frequency of exacerbations in people with COPD and sputum production. However, prescribing antibiotics to large numbers of people could increase levels of antimicrobial resistance, made worse if adherence is poor because patients are not taking antibiotics for current symptoms, and with azithromycin, having to remember to take them 3 times a week. Therefore prophylactic antibiotics are recommended for the people who are likely to benefit from them most, and whose exacerbations are not well managed with other treatments.
Before starting prophylactic antibiotic therapy, consider whether specialist input is needed. The patient should have sputum culture to rule out other possible causes of infections such as TB, atypical mycobacteria or Pseudomonas aeruginosa; training in airways clearance techniques; and a CT scan to rule out bronchiectasis and other lung disease.
Consider azithromycin (usually 250mg 3 times a week) for people with COPD, if they:
- Do not smoke, and
- Have optimised non-pharmacological management and inhaled therapies, relevant vaccinations and been referred for pulmonary rehabilitation, and
- Continue to have 1 or more of the following, particularly if they have significant daily sputum production:
– frequent (4 or more per year) exacerbations with sputum production
– Prolonged exacerbations with sputum production
– Exacerbations resulting in hospitalisation
Azithromycin is associated with a small risk of hearing loss and tinnitus, about which patients should be warned.
Review prophylaxis after the first 3 months, then 6 monthly, and only continue if benefits outweigh risks.
For people who are taking prophylactic azithromycin and who are still at risk of exacerbations, provide a non-macrolide antibiotic to keep at home as part of their exacerbation action plan but there is no need to discontinue the azithromycin during an acute exacerbation.
SUPPLEMENTARY OXYGEN
There is evidence that continuous long term oxygen (O2) therapy improves survival in people with more severe hypoxaemia but not for people with mild hypoxaemia. The evidence also shows the risks of harm from the use of long term O2 therapy, in particular burns and fires as a result of smoking while using oxygen, and falls from tripping over equipment.
NICE has identified two levels of risk:
- COPD patients who do not smoke but who live with people who smoke: Using cigarettes near oxygen could cause fires or burns, but this risk is likely to be lower because the smoker can keep away from the oxygen. These patients may benefit from O2 therapy if they meet the eligibility criteria and the risk assessment is favourable.
- COPD patients who smoke: These patients will be smoking in close proximity to the oxygen and the risks to them and the people they live with outweigh the potential benefits.
Given these risks to the person with COPD and the people they live with, NICE recommends conducting a detailed risk assessment before offering this treatment.
Long term O2 therapy should be considered for patients with severe airflow obstruction (FEV1 30-49% predicted), partial pressure of O2 in arterial blood (PaO2) of7.3 and
Before long term O2 is initiated, there should be a structured risk assessment particularly in relation to smoking – including whether anyone living with the patient smokes. Do not offer long term O2 to people who continue to smoke despite being offered smoking cessation advice and treatment, and referral to specialist stop smoking services.
The 2018 guideline also makes a number of new recommendations on the use of ambulatory O2.
Do not offer ambulatory or short burst O2 to manage breathlessness in people who have only mild or no hypoxia at rest.
Consider ambulatory O2 for people with COPD who have exercise desaturation but whose exercise capacity improves with O2, and who are motivated to use it.
References
1. British Lung Foundation. COPD statistics
2. NICE NG115. Chronic obstructive pulmonary disease in over 16s: diagnosis and management, December 2018. https://www.nice.org.uk/guidance/ng115/
3. NICE NG56. Multimorbidity: clinical assessment and management, 2016. https://www.nice.org.uk/guidance/ng56
Related guidelines
View all Guidelines