E-cigarettes: a Practice Nurse guide
Mandy Galloway
Mandy Galloway
Editor, Practice Nurse and medical writer
This month is Stoptober, the national initiative to encourage people to stop smoking for 28 days, hopefully encouraging them to give up for good. But how should you advise patients who ask about the role of e-cigarettes?
Imagine this: you step into the waiting room and to your horror, you see a young woman taking a deep drag on what at first glance appears to be a cigarette. You immediately approach her to tell her that she cannot smoke here – but she argues, ‘I’m not smoking, I’m only vaping – and you can’t stop me.’
What she says is true – there is currently no ban on using electronic cigarettes, colloquially known as ‘vaping’, in public places. Nonetheless, it would be just as appropriate for you to say that she cannot do so on practice premises, as it would be to ask her to switch off her mobile phone.
This young woman is one of an estimated two million-plus people who use e-cigarettes in the UK.1 The number of users has soared over the past 10 years, and these increasingly popular products have raised a host of questions for Government, healthcare professionals and regulatory authorities alike.
They are portrayed in the media as a healthier choice than conventional tobacco cigarettes, and a way of circumventing smoking restrictions. In surveys, the most common reasons given for trying e-cigarettes are for use in places where smoking is banned, to cut down on smoking and for help with quitting smoking.2
Currently e-cigarettes are regulated solely as a consumer product, but concerns over their safety and quality – as well as uncertainty over their usefulness as aids to smoking cessation – have prompted the UK Government to hand over the regulation of all products containing 20mg/ml nicotine or more to the Medicines and Healthcare products Regulatory Agency (MHRA), to be licensed in the same way as any other medicinal product from 2016.3
WHAT ARE THEY
e-cigarettes are not cigarettes. They do not contain tobacco, and using them is not smoking. e-cigarettes are battery-operated products designed to replicate smoking without the use of tobacco. Some look like conventional cigarettes, while others appear more like an electronic device.
They use heat to vaporise a liquid-based solution containing nicotine into an aerosol mist, hence the term ‘vaping’.
There are three main types – disposable products; an electronic kit that is rechargeable with replaceable, pre-filled cartridges; or a device that has a reservoir, which has to be filled with liquid nicotine. The first two often have a light at the end that glows when the user draws on the device, enhancing their resemblance to a lit cigarette. The level of nicotine varies, and most also contain flavourings. Unlike conventional cigarettes, they do not release a stream of ‘smoke’ but nicotine vapour is released into the air as the user exhales.
VARIABILITY AND SAFETY
There is wide variability in e-cigarette product engineering, including varying nicotine concentrations in the solution used to generate the nicotine aerosol, varying volumes of solution in the product, different carrier compounds, a wide range of additives and flavours, and battery voltage.2
Cytotoxicity also varies among products, from little or none, to highly cytotoxic. They have been marketed as less harmful alternatives to cigarettes but e-cigarette products are highly variable in the efficacy of their vaporization of nicotine, and the labelling of nicotine levels may be inconsistent and misleading.2
The most common carrier liquids are based on propylene glycol (with or without glycerine) and exposure to propylene glycol can cause eye and respiratory irritation. When heated and vaporised, propylene glycol can form propylene oxide, a classified carcinogen.2
An American Foods and Drug Administration (FDA) analysis of two leading brands of e-cigarettes found they contained carcinogens and toxic chemicals, including diethylene glycol, tobacco-specific nitrosamines (human carcinogens) and tobacco-specific impurities suspected of being harmful to humans (anabasine, myosmine and βnicotyrine).4
Compared with second hand smoke, second-hand vapour from e-cigarettes has an overall 10-fold decrease in harmful particles and almost no organic carcinogens, probably because they do not burn organic material.5
But researchers have found that e-cigarette vapour contains chromium – a toxic element that is not present in traditional cigarettes – and nickel at levels four times higher than normal cigarettes. Other toxic metals present in e-cigarette vapour included lead and zinc, although at lower concentrations than in normal cigarettes.5
Among the other chemicals identified in second-hand vapour are formaldehyde, acetaldehyde, isoprene, acetic acid, 2-butanodione, acetone, propanol, propylene glycol, and diacetin.2
However, writing in the British Journal of General Practice last month Professor Robert West and Dr Jamie Brown from University College London say that despite alarmist commentaries, studies on the toxicology of the vapour tell us that, while propylene glycol is an irritant and some toxins are present in measurable quantities, the concentrations are very low, less than 1/20th of that of cigarette smoke.6
SMOKING CESSATION
e-cigarettes have been proposed as a way to help smokers quit the habit, but the jury is still out on whether or not they are effective.
West and Brown claim that for every million smokers who switch from tobacco to e-cigarettes, over 6,000 premature deaths would be prevented in the UK every year. If all 9 million smokers took up e-cigarettes instead, 54,000 lives could be saved.6 They point out that ‘people smoke for the nicotine but die from the tar.’
Two randomised controlled trials of e-cigarette products containing low levels of nicotine found quit rates similar to those of licensed nicotine products. However, the latest study on the effectiveness of e-cigarettes as an aid to smoking cessation, published last month in the journal, Addiction, found that smokers who used these products were more than one-and-a-half times more likely to quit than those who used NRT bought over the counter or tried to give up unaided.7
The study included 5,863 adults who had smoked within the previous 12 months and made at least one quit attempt during that period with either an e-cigarette only (n = 464), NRT bought over-the-counter only (n = 1922) or no aid in their most recent quit attempt (n = 3477).
Among smokers who attempted to stop without professional support, those who used e-cigarettes were more likely to report continued abstinence than those who used a licensed NRT product bought over-the-counter or no aid to cessation. This difference persisted after adjusting for a range of smoker characteristics such as nicotine dependence.7
UNDOING THE GOOD WORK?
There is widespread concern that the growing popularity of e-cigarettes may help to ‘re-normalise’ smoking.
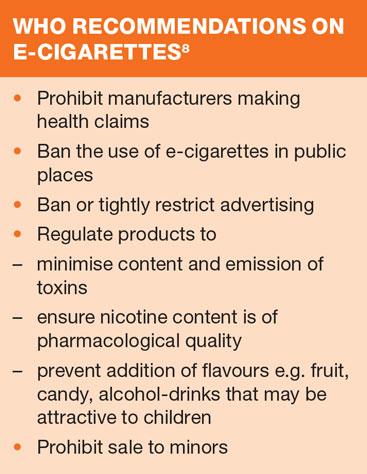
The recent World Health Organization report on electronic nicotine delivery systems (ENDS) states: ‘This renormalisation effect refers to the possibility that everything that makes ENDS attractive to smokers may enhance the attractiveness of smoking itself and perpetuate the smoking epidemic. ENDS mimic the personal experience and public performance of smoking and their market growth requires marketing that is challenging barriers erected to prevent the promotion of tobacco products.’8
WHO is also concerned that allowing use of e-cigarettes in places where smoking is banned reduces the incentive for smokers to quit and undoes the ‘de-normalising effects’ of smoking bans.
This concern relates predominantly to young people, who are particularly susceptible to visual cues and social norms.8
There are also concerns about young people’s use of e-cigarettes despite never having previously smoked tobacco.2 Dual use of e-cigarettes and conventional cigarettes is common, and there is an increasing body of evidence that shows young people who experiment with e-cigarettes have never tried a tobacco cigarette, thus initiating use of nicotine (an addictive drug) with the electronic product.2
Professor John Ashton, of the Faculty of Public Health, said: ‘We don’t know enough yet about the harms and side effects of electronic cigarettes, and it will take years before we can be sure what they are. Public health experts are concerned that those harms could include a “gateway effect”, which will mean that young people will become addicted to cigarettes after initially using electronic devices.'9
In contrast, West and Brown point out that warnings about a rapid rise in e-cigarette use among the young have been based on the proportion of young people who report ever having tried an e-cigarette, not the proportion of current users, and that the proportion of current e-cigarette users in England who have not smoked regularly is ‘extremely small’, at 0.2%.6
ADVICE TO HEALTH PROFESSIONALS
In the light of the lack of scientific evidence on the efficacy and safety of e-cigarettes, health professionals should encourage their patients to use a regulated and licensed nicotine replacement therapy to help quit smoking. Where a patient is unable or unwilling to use or continue to use an approved and tested NRT, practice nurses should advise patients that while e-cigarettes are unregulated and their safety cannot be assured, they are likely to be a lower risk option than continuing to smoke.4
REFERENCES
1. Action on Smoking and Health (ASH). Briefing: Electronic cigarettes, June 2014. http://www.ash.org.uk/files/documents/ASH_715.pdf
2. Grana R, Benowitz N, Glantz S. E-Cigarettes: a scientific review. Circulation 2014;129:1972-86
3. MHRA. UK moves towards safe and effective electronic cigarettes and other nicotine containing products. Press Release, June 2013. http://www.mhra.gov.uk/NewsCentre/Pressreleases/CON286855
4. BMA briefing paper, March 2012 (updated 2013) http://bma.org.uk/working-for-change/improving-and-protecting-health/tobacco/e-cigarettes
5. Saffari A, Daher N, Ruprecht A, et al. Particulate metals and organic compounds from electronic and tobacco-containing cigarettes: comparison of emission rates and secondhand exposure. Environ Sci Processes Impact 2014;DOI: 10.1039/C4EM00415A
6. West R, Brown J. Electronic cigarettes: fact and faction. BJGP 2014; DOI:10.3399/bjgp14X681253 http://bjgp.org/content/64/626/442
7. Brown J, Beard E, Kotz D, et al. Real-world effectiveness of e-cigarettes when used to aid smoking cessation: a cross-sectional population study. Addiction 2014;9:1531-1540
8. WHO. Electronic nicotine delivery systems, July 2014. http://apps.who.int/gb/fctc/PDF/cop6/FCTC_COP6_10-en.pdf
9. Faculty of Public Health. Press statement, 27 August 2014. http://www.fph.org.uk/who_approach_to_e-cigarettes_good_news_for_children’s_health,_says_fph