
Obesity management: the roles of GLP-1 RAs and behaviour change
Jane DeVille-Almond
Jane DeVille-Almond
SRN, SCM, HV, BA (Hons) Cert Ed
President of the British Obesity Society
Practice Nurse 2025;55(1):22-26
It may be tempting to rely on recently recommended drug therapies to help patients lose weight, but effective management of obesity requires a dual approach including both lifestyle changes and pharmacotherapy
In the ever-evolving landscape of healthcare, obesity management stands as one of the most pressing challenges faced by primary care providers, with around 29% of adults classified as obese and an additional 35% overweight.1 As we explore the complexities of this multifaceted issue, it becomes increasingly clear that effective management may include a dual approach incorporating both lifestyle changes and innovative pharmacological solutions, such as glucagon-like peptide-1 receptor agonists (GLP-1 Ras), used in conjunction with robust behaviour change strategies.
LEARNING OBJECTIVES
After reading this article you should be better informed about:
- The definition of, and factors contributing to, obesity
- Strategies to help patients lose weight and advice for achieving weight loss
- The role of current pharmacological interventions and recommendations for use
- The importance of behaviour change
The government also realises the need to target the food industry which currently spends billions of pounds each year to encourage us to buy foods that are ultimately harming our health. Over the years the government has developed policies that will ban the advertising of unhealthy foods high in fat salt and sugar (FHSS) especially to children and young people, but these have not yet to be implemented. Legislation that was due to come into force from 1 January 2023 has been delayed to 1 October 2025. This legislation includes banning volume promotions of unhealthy foods such as ‘buy one get one free’ offers’ and prohibiting food advertising before the 9pm watershed.2
THE OBESITY EPIDEMIC: A CALL TO ACTION
Obesity is defined by a Body Mass Index (BMI) of 30 kg/m2 or higher (27.5 in the Asian population). NICE guidelines also suggest waist measurements should be used in conjunction with a BMI below 35 kg/m2 to measure central adiposity.3
Obesity is not merely a matter of excess weight; it is a chronic disease that significantly elevates the risk of comorbidities, including type 2 diabetes, hypertension, cardiovascular disease and several cancers. The rise in obesity rates can be attributed to factors such as sedentary lifestyles, poor dietary habits, genetic predispositions and easy access to ultra processed foods (UPF). According to the World Obesity Federation, the prevalence of obesity has tripled since 1975, emphasising the urgent need for effective interventions within primary care.4
General practice nurses are uniquely positioned to address this epidemic through patient education, tailored management plans that resonate with a patients' individual needs, and ongoing support. However, healthcare professionals must be realistic about the time available for such services, so it is imperative that they make the most of the initial consultation and encourage the patient to accept an element of personal responsibility.
INITIAL ASSESSMENT
Achieving weight loss without the use of drugs can be a highly effective approach for many individuals, and there are several evidence-based strategies that focus on lifestyle changes. These include food, drink and exercise tracking, dietary adjustments and behaviour modification. Initial assessments of patients should include:
- Establishing the motivation, capability and opportunity of your patient. Are they ready and willing to make changes?
- Measuring height and weight. Many patients guess their height and weight which may alter their own calculation of BMI
- Calculate BMI
- Take waist measurements of those with a BMI less that 35 kg/m2. This will help provide a practical measurement of central adiposity. The waist should measure no more than half a person’s height. People with high levels of fat around their abdomen are more likely to develop weight related conditions.3
- Calculate Basal Metabolic Rates (BMR) (available at https://www.calculator.net/bmr-calculator.html) This calculates the minimum number of calories our body needs, while resting, to maintain its basic functions. It is a useful guideline for your patients to understand how many calories their body requires in a day. To lose weight these calories need to be reduced.
- Assess lifestyle factors such as eating habits, physical activity levels and psychosocial factors that may be contributing to their obesity.
It’s important that HCPs have established these factors before collaborating with patients to design individual care plans, as it is clear not one size fits all.
ADVICE FOR ACHIEVING WEIGHT LOSS
- Prioritise sleep: Quality sleep is crucial for weight management, as research indicates that lack of sleep disrupts hormones related to hunger. Lack of sleep may lead to increased appetite and cravings for unhealthy foods. Patients should aim for 7-9 hours of quality sleep to improve weight loss outcomes.5 Strategies to improve sleep include:
- Establishing a regular sleep pattern where possible (be aware that many people work unsociable hours)
- Creating a relaxing bedtime routine (if possible) this would include limiting screen time before bed
- Read a book or listen to relaxing music before bedtime
- Practise relaxation techniques (podcasts might help)
- Try sleeping in a dark, cool room.
- Mindful eating: means paying attention to what you are eating and why, and trying to recognise hunger, and satiety cues. Encourage those who have a smart phone to use a free app such as NHS weight loss, or MyFitnessPal, to help achieve their goals. Suggest eating meals at a table, where possible, and discourage eating while doing other things such as driving, watching TV or working at a computer or phone.
- Hydration: Staying well hydrated is essential for weight loss. If people are thirsty, they should drink water. Thirst is often mistaken for hunger. High calorie drinks should be a treat and not used for quenching thirst. Even low-calorie drinks may cause a craving for sweet high calorie foods and end up adding to weight gain.6 Remind people of the high calorie content of sugary drinks, alcohol, and some coffees as these often contribute significantly to weight gain.
- Portion Control: In a recent study carried out by MyFitnessPal and the British Obesity Society it was found that around 50% of people that took part did not know how to measure a portion of rice, pasta or cereals. Many people use double or triple the recommended servings, which leads to higher calorie consumption, and can contribute to weight gain. Using smartphone apps will help patients recognise a portion.
- Focus on whole foods: Eating whole, minimally processed, foods can aid in weight loss, due to their nutritional density and lower calorie content compared to processed foods.
- Increase protein intake: Higher protein diets have long been encouraged to prevent or treat obesity.7 High protein foods can enhance satiety which helps reduce overall calorie intake. Protein has a higher thermic effect compared with fats and carbohydrates, meaning the body burns up more fat just digesting the protein. Protein-rich foods include lean meats such as chicken and turkey, fish, eggs, legumes (beans, lentils), nuts.
- Increase fibre intake: Studies have found that dietary fibre not only promotes feelings of fullness and aids digestion but is also associated with weight loss.8 High fibre foods include fruits, vegetables, whole grains, and legumes such as beans and lentils.
- Physical activity: NICE suggests that adults trying to lose weight should do at least 30 minutes of moderate physical activity at least 5 days a week, and in some cases up to 45-60 minutes, for it to have an impact.9 Activity can be broken up into shorter sessions. Examples of moderate activity include gardening, brisk walking, swimming, exercise classes, cycling, climbing stairs. Note that exercise alone is not as effective as combining it with cutting calories, and that cutting calories has the most impact. Exercise helps maintaining a healthy weight, and is also good for heart, lung, joint and mental health.
- Managing stress: Chronic stress can lead to cravings and overeating due to elevated cortisol levels, which promote fat storage, particularly around the abdomen. HCPs should encourage patients to engage in practising mindfulness, meditation, deep breathing, relaxation exercises such as yoga, and hobbies or activities that provide joy and relaxation.
- Regular weighing: Research shows that patients who weigh themselves regularly, more than once a week, are more likely to be successful in losing and maintaining weight.10 Many patients avoid their scales when they know they have gained weight, so it’s important to encourage patients to weigh themselves regularly. Remind them it is far easier to lose a 1lb gained than to lose half a stone. The surgery should not be somewhere people come to get weighed, unless there are scales outside a consulting room, as this is a very expensive service to offer. Encourage patients to invest in good quality scales.
THE ROLE OF PHARMACOLOGICAL INTERVENTIONS
In recent years, GLP-1 RAs have emerged as a groundbreaking class of medications for obesity management. These agents - such as semaglutide (Wegovy®), liraglutide (Victoza® and Saxenda®) and the combination glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 receptor agonist, tirzepatide (Mounjaro®) – work by mimicking the incretin hormones that the body naturally produces in response to food intake. They promote satiety, reduce appetite, and enhance glycaemic control, making them particularly beneficial for individuals with obesity and type 2 diabetes.
The results of recent clinical trials are impressive, with patients experiencing significant weight loss and improved metabolic outcomes. For instance, the STEP trials demonstrated that participants receiving once weekly subcutaneous semaglutide, in conjunction with lifestyle modifications, achieved an average weight loss of around 15% over 68 weeks.11 Such outcomes are encouraging, but they also raise important questions about accessibility, adherence, and the role of healthcare providers in guiding patients through their weight loss journeys.
Semaglutide
NICE recommends semaglutide as an option for weight management, including weight loss, alongside reduced calorie diet and increased physical activity,12 for adults with:
- At least one weight-related comorbitity
- BMI of at least 35.0kg/m2, or
- BMI of 30.0–34.9 kg/m2 and meet the criteria for referral to specialist weight management services
Semaglutide is only approved for a maximum of 2 years and available via specialist weight management services, which provide multidisciplinary management of overweight or obese adults.
Tirzepatide
NICE has approved tirzepatide as an option for managing overweight and obesity alongside a reduced-calorie diet and increased physical activity,13 but with strict pre-conditions.
Tirzepatide will not be available to everyone immediately, as NICE has agreed with NHS England on a slow roll-out over 12 years to protect services in the NHS.
It will initially be offered to those patients with a BMI over 35 kg/m2 (reduced by 2.5 kg/m2 for people from Asian, Black African or African-Caribbean ethnic backgrounds) with at least one comorbidity. Initially, this will be fewer that 10% of all those in England who are eligible for the drug.
NHSE justified its request for a delay to full implementation on the grounds that:
- Weight management services are not routinely commissioned in primary care, and time was needed to develop services
- There is insufficient capacity to deliver tirzepatide in primary care, and healthcare professionals will require training
- If an extension to the time required to implement NICE’s recommendations was not granted, existing services would need to be decommissioned to release resources to deliver tirzepatide.
The cost of implementing NICE recommendations in full is anticipated to be more than £20m in each of the first 3 years. Integrated care boards (ICBs) will be required to fund tirzepatide within 3 months for patients accessing specialist weight management services, and from 6 months to support a phased introduction.
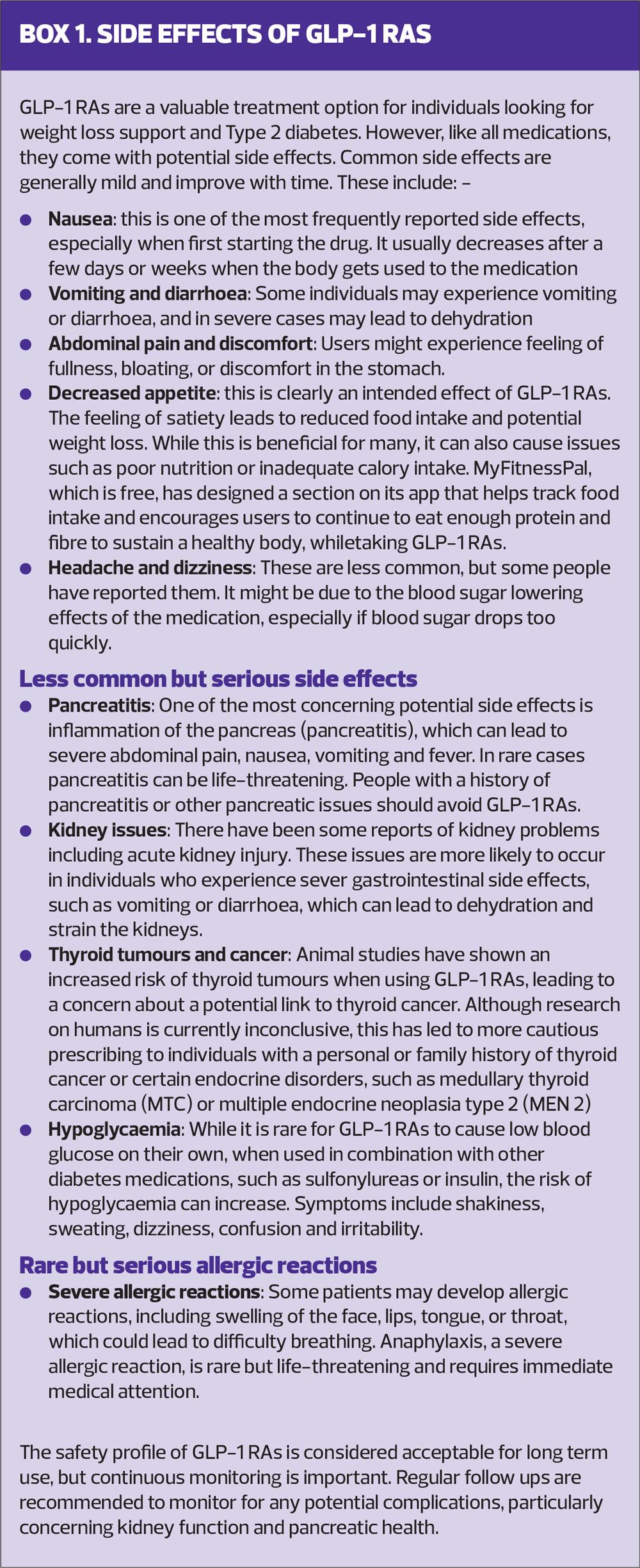
It should be remembered that these pharmacological interventions do not come without side effects, which may be serious in some cases (Box 1). It is therefore crucial to emphasise to patients the importance of having these drugs prescribed by a registered medical professional, who will monitor their progress, and not obtain them online.
THE ROLE OF BEHAVIOUR CHANGE
While GLP-1 medications offer a promising pharmacological option, they are not a panacea for obesity management. Behaviour change remains a cornerstone of effective treatment, necessitating a holistic approach that empowers patients to take charge of their health.
As healthcare professionals, we must adopt a compassionate, patient-centred approach to facilitate behaviour change. Here are several strategies that can be woven into the fabric of our practice:
1. Motivational Interviewing: This patient-centred counselling style encourages individuals to explore and resolve ambivalence about change. By fostering an open dialogue, we can help patients identify their motivations for weight loss and health improvement.
2. Goal Setting: Collaboratively setting realistic, achievable, measurable goals can enhance patient engagement and accountability. Focusing on small, incremental changes – such as increasing physical activity or improving dietary choices – can lead to sustainable weight loss over time.
3. Support Systems: Encouraging patients to seek support from family, friends, or community resources can bolster their efforts and improve outcomes.
4. Education and resources: Equipping patients with knowledge about nutrition, physical activity, and mindfulness, can empower them to make informed choices.
NHS Digital programme
General practices and community pharmacies can refer members of the public to the NHS Digital Weight Management Programme. This is a 12-week online behavioural and lifestyle programme, which people can access online. To be referred, patients must be:
- 18 or over.
- Have a BMI greater than 30 kg/m2 (27.5 kg/m2 for people from black, Asian, and ethnic minority backgrounds, as we know people from these ethnic backgrounds are at an increased risk of conditions such as type 2 diabetes at a lower BMI).
- Have diabetes, hypertension, or both.
- Have a smartphone, tablet, or computer with internet access.
INTEGRATING MEDICATIONS WITH BEHAVIOUR CHANGE
The integration of GLP-1 RAs and GIP/GLP-1 RAs into a comprehensive obesity management plan should be approached with a clear understanding of the patient’s context. It is essential to discuss both the potential benefits and side effects of these medications, ensuring that patients have realistic expectations. Moreover, combining pharmacotherapy with behaviour change interventions can lead to improved outcomes. For instance, a patient who is actively engaged in lifestyle changes may find it easier to adhere to a medication regimen and vice versa.
CONCLUSION: A COLLABORATIVE EFFORT
Managing obesity in primary care is a complex yet rewarding endeavour. The advent of effective weight-loss medications has provided us with a powerful tool, but it is the synergy of pharmacological and behavioural interventions that will ultimately pave the way for success. As we continue to address the obesity epidemic, let us remain committed to fostering a supportive environment for our patients – one that embraces both the science of medication and the art of behaviour change.
In this collaborative effort, nurses play a pivotal role as educators, motivators, and advocates. By harnessing our expertise and compassion, we can empower our patients to embark on sustainable journeys towards better health – one small step at a time.
REFERENCES
1. NHS England. Health Survey for England, 2021, Part 2;2023 https://www.gov.uk/government/statistics/health-survey-for-england-2021-part-2
2. UK Government. Consultation outcome; September 2024. https://www.gov.uk/government/consultations/introducing-further-advertising-restrictions-on-tv-and-online-for-products-high-in-fat-salt-or-sugar-secondary-legislation/outcome/introducing-further-advertising-restrictions-on-tv-and-online-for-products-high-in-fat-salt-or-sugar-government-response-to-consultation-on-secondary-legislation
3. NICE. Keep the size of your waist to less than half of your height, (press release); April 2022
4. World Obesity. Prevalence of obesity. https://www.worldobesity.org/about/about-obesity/prevalence-of-obesity
5. Cooper CB, Neufeld EV, Dolezal BA, et al. Sleep deprivation and obesity in adults: a brief narrative review. BMJ Open Sports Exerc Med 2018;4:e000392 https://bmjopensem.bmj.com/content/bmjosem/4/1/e000392.full.pdf
6. Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review, Am J Clin Nutr 2006;84(2):274-288 https://pmc.ncbi.nlm.nih.gov/articles/PMC3210834/
7. Leidy HJ, Clifton PM, Astrup A, et al. The role of protein in weight loss and maintenance. Am J Clin Nutr 2015 Jun;101(6):1320S-1329S. https://pubmed.ncbi.nlm.nih.gov/25926512/
8. Kelly RK, Calhoun J, Hanus A, et al. Increased dietary fiber is associated with weight loss among Full Plate Living program participants. Front Nutr 2023; 10:1110748.
9. NICE PH44. Physical activity: brief advice for adults in primary care; 2013. https://www.nice.org.uk/guidance/ph44
10. Vuorinen A, Helander E, Pietilä J, et al. Frequency of Self-Weighing and Weight Change: Cohort Study With 10,000 Smart Scale Users, J Med Internet Res 2021;23(6):e25529 https://www.jmir.org/2021/6/e25529/
11. Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. https://pubmed.ncbi.nlm.nih.gov/35015037/
12. NICE TA875. Semaglutide for managing overweight and obesity; 2023. https://www.nice.org.uk/guidance/TA875/
13. NICE. Tirzepatide for managing overweight and obesity. December 2024. https://www.nice.org.uk/guidance/indevelopment/gid-ta11156
Related articles
View all Articles