Eating disorders – management in primary care
DR GERRY MORROW MB ChB, MRCGP, Dip CBT
DR GERRY MORROW MB ChB, MRCGP, Dip CBT
Medical Director and Editor, Clarity Informatics Limited
Eating disorders are rare in the general population, but are a common condition in young women, with a high risk of psychiatric comorbidity and mortality. Practice nurses need to have a raised index of suspicion of these conditions to detect them early and refer appropriately
An eating disorder is characterised by a persistent disturbance of eating or eating related behaviour that results in altered consumption that significantly impairs physical health or psychosocial functioning.1
Eating disorders can be subdivided as follows:
- Anorexia nervosa – a low body weight as a result of a preoccupation with weight, construed as either a fear of fatness or a pursuit of thinness
- Bulimia nervosa – recurrent episodes of binge eating and compensatory behaviour (any one of, or a combination of vomiting, fasting, or excessive exercise)
- Binge eating disorder – recurring episodes of eating significantly more food in a short period of time than most people would eat under similar circumstances. There is no compensatory behaviour
- Atypical eating disorders – an eating disorder which does not meet precise diagnostic criteria.
The cause of eating disorders is multifactorial.2 The main risk factors for developing eating disorders include:
- General factors – female sex, adolescence and early adulthood, western society
- Family history – of an eating disorder of any type, depression, or substance misuse
- Premorbid experiences – sexual abuse, criticism regarding eating or body shape and weight, preoccupation with slimness, occupational or recreational pressure to be slim
- Premorbid characteristics – low self-esteem, perfectionism, anxiety disorders, obsessional personality, borderline personality disorder, obesity, early menarche, or difficulty resolving conflict.
Eating disorders are rare, however they are relatively common in teenagers and young women. They are thought to be the third most common chronic illness (after asthma and obesity) in adolescent females.
Atypical eating disorders are the most common presentation, followed by binge eating disorders, and bulimia nervosa. Anorexia nervosa is the least common.
The incidence of atypical eating disorders is 40 to 50 in 1,000 people per year, more commonly in females than males.
The incidence of binge eating disorders is 16 in 1,000 females per year.
The incidence of bulimia nervosa has been estimated to be between 10 to 15 in 1,000 of females per year.
The incidence of anorexia nervosa is 0.4 in 1,000 females per year. 9 in 1,000 females will experience anorexia at some point in their lives. It is less common in males than females.3
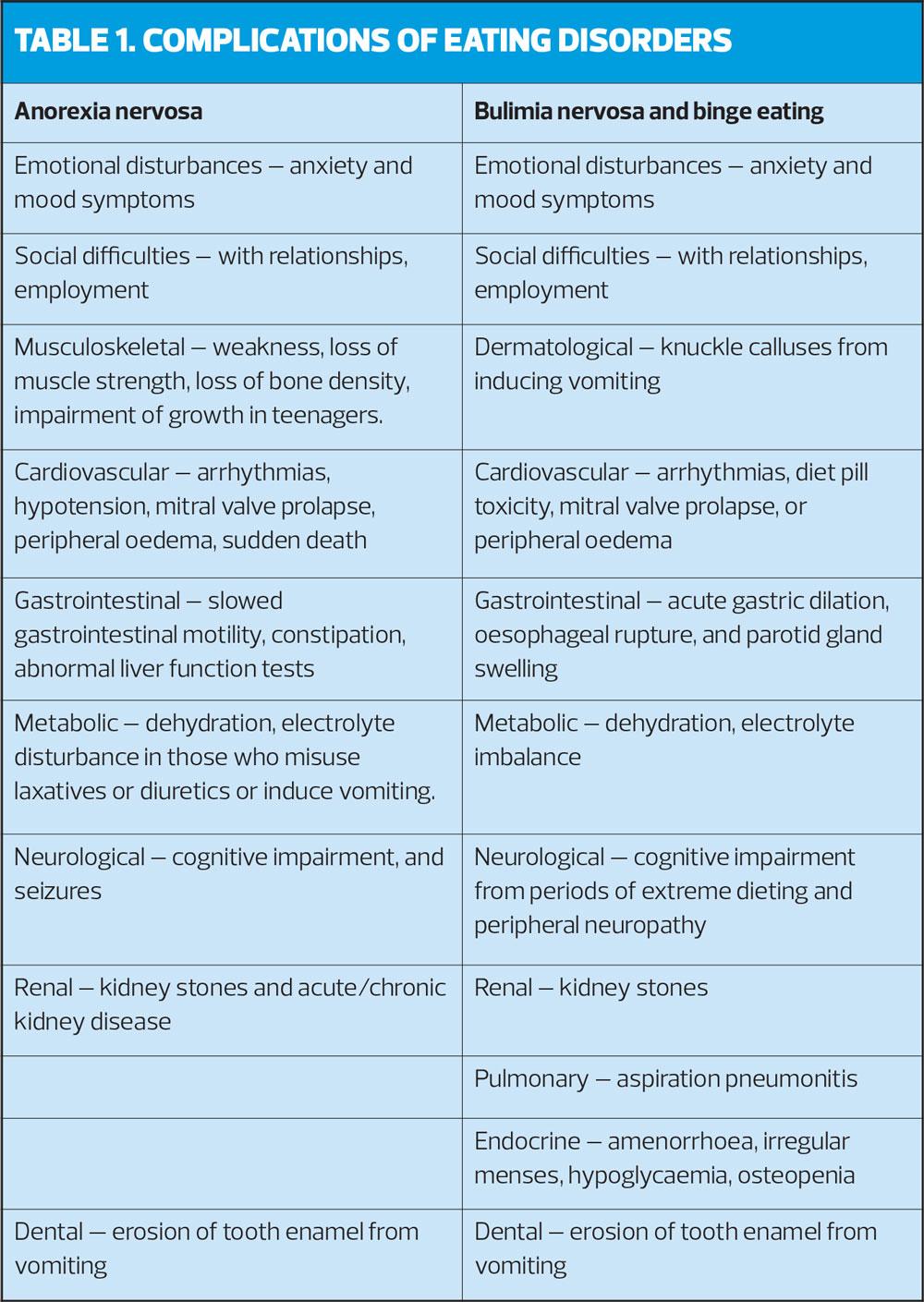
COMPLICATIONS
Anorexia nervosa
Physical abnormalities seen in anorexia nervosa are usually secondary to starvation and are usually reversible once normal eating and good nutrition are resumed (Table 1).
Bulimia nervosa and binge eating
Physical abnormalities seen in people with bulimia nervosa and binge eating are usually minor compared with those found in anorexia unless vomiting, laxative, or diuretic misuse is frequent (Table 1).
Atypical eating disorders
Atypical eating disorders are characterised by symptoms of an eating disorder but do not meet the precise diagnostic criteria for them. For example, in anorexia nervosa, there is significant weight loss, but the person's weight is within or above normal range.
WHAT IS THE PROGNOSIS?
Anorexia nervosa
The course of anorexia nervosa is very variable. However, recovery from anorexia nervosa becomes less likely the longer the person has the illness.
Approximately 50% of people with anorexia nervosa completely recover, 33% improve, and 20% develop a chronic eating disorder. The risk of death in people with anorexia nervosa is increased due to medical complications and suicide. The mortality rate of people with anorexia nervosa has been estimated to be 2.8%. This is three times higher than for any other psychiatric illness.
Bulimia nervosa
Compared with anorexia nervosa, bulimia nervosa is associated with better recovery rates and lower mortality rates. Approximately 70% of people with bulimia nervosa recover over time.
Binge eating disorder
Less is known about binge eating disorders. However, it is thought that approximately 70–80% of people with binge eating disorders will recover over time. The course of binge eating disorder is similar to that of bulimia nervosa. Cross over from binge eating to other eating disorders is rare.
Atypical eating disorders
The prognosis depends largely on the severity of associated physical and psychological features.4
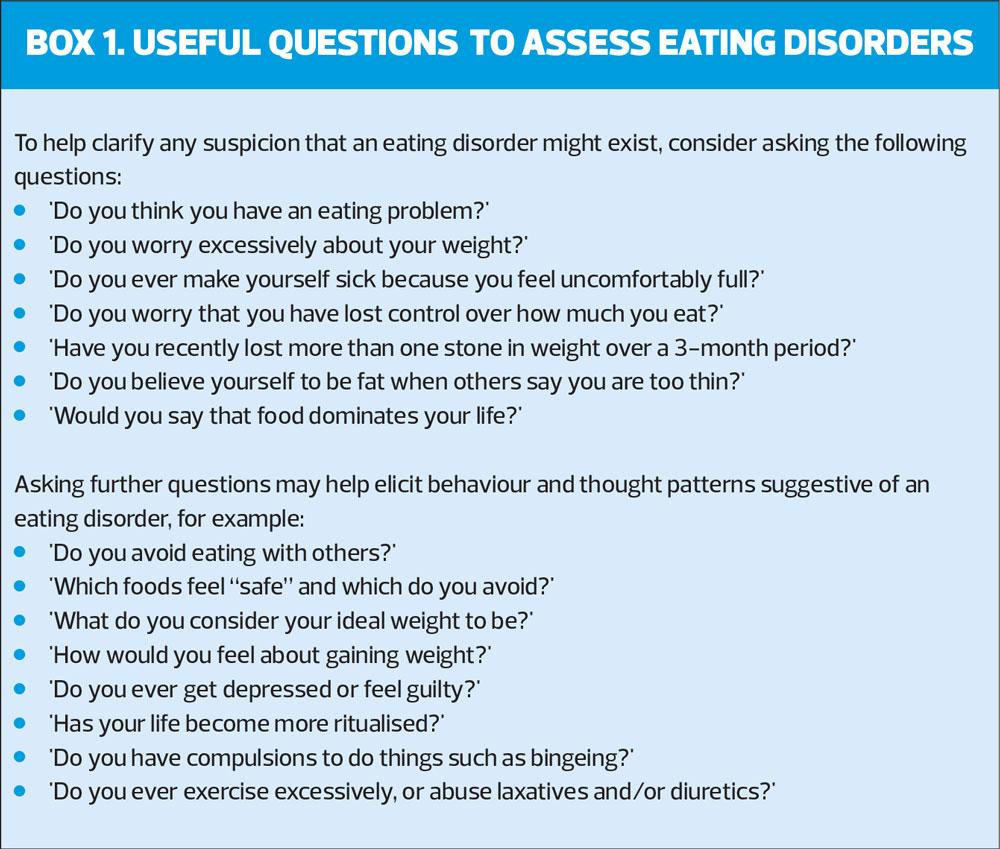
DIAGNOSIS OF EATING DISORDERS
The diagnosis of an eating disorder is made on the basis of the person's history, the suggestive clinical features (see below), and where possible, by corroboration from a relative or friend.
Be aware that eating disorders are often difficult to detect in primary care, as people are slow to present and may only do so when persuaded by concerned family members or friends, and may present with non-specific symptoms, such as fatigue or dizziness.
Have a lower threshold for suspecting an eating disorder in:
- Young women with low body mass index (this should not be used in isolation to determine the offer of treatment)
- People consulting with weight concerns who are not overweight, or who are underweight
- Women with menstrual disturbances or amenorrhoea
- People with gastrointestinal symptoms, such as constipation, bloating, and gastro-oesophageal reflux
- People with physical signs of starvation or repeated vomiting
- Young people with type 1 diabetes and poor treatment adherence
- Children with poor growth
- Women with psychological or psychiatric illness should be considered at higher risk of an eating disorder.
Anorexia nervosa
Clinical features of anorexia nervosa include maintaining weight at least 15% below that expected for the person;5,6 (in adults this normally represents a body mass index [BMI] of less than 17.5 kg/m2); and avoidance of foods thought to be fattening to achieve weight loss. One or more of the following compensatory behaviours may also be present:
- Self-induced purging (vomiting or excessive use of laxatives)
- Excessive exercise
- Use of appetite suppressants
- Use of diuretics.
Anorexia nervosa is also associated with a number of psychological features, which may include:
- Distortion of body image, with a dread of fatness
- Over-evaluation of self-worth in terms of weight and shape
- Weight loss viewed as a positive achievement
- Denial of the seriousness of the weight loss and impact on physical health
- Difficulty acknowledging there is a problem.
Physical features can include a widespread endocrine disorder, amenorrhoea in women and erectile dysfunction in men. Before puberty, growth and physical development can be affected. Other symptoms, such as constipation, headache, fainting, dizziness, fatigue, and cold intolerance may be present. Physical signs include cachexic appearance, hands or feet are red or purple in colour, dry skin, hair loss, bradycardia, orthostatic hypotension, hypothermia, loss of muscle mass and subcutaneous fat, oedema, and downy hair on the upper part of the body and face.
Bulimia nervosa
Bulimia is characterised by recurrent episodes of binge eating (in a defined period of time [typically within a 2-hour period], much more than most people would eat under similar circumstances) which occur with feelings of loss of control over how much is being eaten, followed by compensatory behaviour (any one of, or a combination of vomiting, purging, fasting, or excessive exercise) in order to prevent weight gain. Purging includes misuse of laxatives or diuretics. Other drugs involved can include thyroxine, amphetamines, or other medication. BMI is generally above 17.5 kg/m2 in adults, although there may be a history of an earlier episode of anorexia nervosa.
Psychological features typically include a fear of gaining weight, with a clearly defined weight self-imposed threshold; self-evaluation unduly influenced by weight and body shape; mood disturbance and symptoms of anxiety; and persistent preoccupation and craving for food and feelings of guilt and shame. Self-harm is also common.
Physical symptoms may include feelings of bloating or fullness, lethargy, gastro-oesophageal reflux, abdominal pain, and sore throat (from vomiting). Physical signs, in severe cases, include knuckle calluses, dental enamel erosion, and salivary gland enlargement.
Binge eating disorder
Clinical features include recurrent episodes of binge eating, which occur with feelings of loss of control over how much is being eaten. Compensatory behaviour (anyone or a combination of vomiting, purging, fasting, or excessive exercise) is absent. Episodes are associated with at least three of the following:
- Eating much more rapidly than normal and until feeling uncomfortably full even when not hungry
- Eating alone because of feeling embarrassed about how much is being eaten
- Feelings of disgust, depression, or guilt afterwards
- Body weight that may be maintained at normal, or the person may be overweight or obese.
- Marked distress regarding binge eating, and social avoidance.
Most eating disorders encountered in the community are atypical.
An eating disorder is described as ‘atypical’ if it has features that closely resemble anorexia nervosa, bulimia nervosa, or binge eating disorder but does not meet the precise diagnostic criteria. Many people with atypical eating disorders have experienced anorexia or bulimia nervosa in the past or may subsequently go on to develop the full syndrome of anorexia or bulimia nervosa.
WHAT ELSE MIGHT IT BE?
There are a large number of causes of weight loss or amenorrhoea, but in practice, eating disorders should be relatively easy to differentiate from other causes. Practice nurses should be aware that the differential diagnosis of weight loss includes malabsorption (for example due to coeliac disease, inflammatory bowel disease), cancer and illicit drug use or alcohol misuse, and hyperthyroidism.
HOW SHOULD I MANAGE A SUSPECTED EATING DISORDER?
First, practice nurses should consider a physical and psychosocial assessment of all people with a suspected eating disorder.
In most people with an eating disorder, investigations will show normal laboratory results. However, some investigations may be useful to rule out complications in people with anorexia nervosa, and to check fluid and electrolyte balance in people with bulimia nervosa.
Consider hospital admission for people who are particularly at risk of physical or psychological complications. For all other people with a suspected eating disorder, refer for specialist assessment and management to a community mental health team, child and adolescent service, or a specialist eating disorder unit.
The urgency of referral will depend on the person's circumstances and on clinical judgement.
If there is uncertainty with regards to the urgency of referral or risk, speak to a GP colleague or contact the nearest specialist eating disorders service for advice.
People with eating disorders should receive treatment at the earliest opportunity. This is particularly important for people with diabetes mellitus and pregnant women, as these groups require increased monitoring.
If anorexia nervosa is suspected:
- Enquire about symptoms, for example menstruation patterns, muscle weakness, cold sensitivity, sleep disturbance, fainting or dizzy spells, and dental problems
- Measure the person's height and weight
- Ideally the person should be weighed before referral. Be aware that some people are so concerned by unwanted interventions by healthcare professionals that they will falsify their weight by drinking copious amounts of water or by hiding heavy objects in clothing
- Calculate the person's body mass index
- Measure core temperature
- Examine the peripheries (for circulation and oedema).
- Perform a cardiovascular examination, including checking for postural hypotension.
Findings on examination may be normal, especially if it is early in the course of the illness.
Performing a psychosocial assessment
Ask about:
- How important it is for them to change their eating patterns
- What they like and dislike about their current eating habits
- The perceived benefits and disadvantages of changing their current habits
- Explore and highlight any problems that their eating or weight loss may be causing them
- Assess for risk of suicide or self-harm, which determines the urgency of referral to specialist mental health services
- Assess for the presence of a psychiatric co-morbidity
- Enquire about the person's level of social support.
What investigations should I request?
Extensive laboratory investigation is not usually required in a primary care setting. Many test results remain normal even with extreme weight loss, however these tests may be useful to rule out complications.
Depending on the results of the history and physical examination, consider the following investigations in primary care
- Full blood count — may show anaemia, mild leucopenia or thrombocytopenia from malnutrition
- Erythrocyte sedimentation rate (ESR) — usually normal in people with anorexia, a raised ESR may indicate an organic cause of weight loss
- Urea and electrolytes — hypokalaemia (potassium level < 3.5 mmol/l) is suggestive of vomiting or laxative abuse; hyponatraemia may be a result of excess water intake
- Creatinine, and urinalysis
- Liver function tests
- Random blood glucose
- Electrocardiography (ECG) — this should be considered for all people with anorexia nervosa
Further tests may be required in more severe cases or to assess complications:
- Calcium, magnesium, phosphate – uncommon problems
- Serum proteins (albumin usually normal unless chronic), creatine kinase
For people with suspected bulimia nervosa with frequent vomiting, or who are taking large quantities of laxatives (especially if they are underweight, check fluid balance and urea and electrolytes.
Other tests include an assessment of bone density,7 but the main way of preventing and treating low bone mineral density is reaching and maintaining a healthy body weight or BMI for their age.
NICE advises clinicians to consider a bone mineral density scan:
- After 1 year of underweight in children and young people, and after 2 years in adults, or earlier if they have bone pain or recurrent fractures
When should I admit a person with a suspected eating disorder?
Consider admission to hospital if any of the following are present
- Risk of suicide or severe self-harm
- Home environment impedes recovery
- Severe deterioration
- Very low body weight (BMI <17.5 kg/m2) or rapid weight loss. Urgent referral is required for anyone with a BMI <15 kg/m2
- Medical complications (for example pronounced oedema, severe electrolyte disturbance, bradycardia, hypoglycaemia, or severe intercurrent infection).
If considering compulsory admission (regardless of the person's age), consider seeking advice from a GP colleague or appropriate specialist.8
How should I manage someone with a confirmed eating disorder?
Advise people who are vomiting on the importance of regular dental review and dental hygiene.
They should avoid brushing their teeth for at least an hour after vomiting (if the teeth are brushed immediately after vomiting, acid is brushed on to the teeth causing further damage); rinse with water or a non-acidic mouthwash after vomiting; and reduce the acidity of the oral environment (for example, by limiting acidic foods).
Record an alert in the prescribing record of people with anorexia nervosa concerning the potential risk of drug adverse effects.
If the person has chronic anorexia nervosa and is not under secondary care, practice nurses should review their physical and mental health at least annually in primary care.
CONCLUSION
Eating disorders although rare in the general population, are the third most common long-term condition in young women, with a high risk of psychiatric comorbidity and mortality. The presentation in primary care may be subtle and involve discussions of a myriad of early symptoms during routine clinical contact with a practice nurse, e.g. contraception reviews and cervical screening. Practice nurses should therefore have a raised index of suspicion of these conditions in order to detect early and refer accordingly.
REFERENCES
1. NICE Clinical Knowledge Summaries Eating Disorders: https://cks.nice.org.uk/eating-disorders#!scenario
2. Fairburn CG, Harrison PJ. Eating disorder. Lancet 2003;361(9355):407-416.
3. Steinhausen HC. The outcome of anorexia nervosa in the 20th century. Am J Psychiatry 2002;159 (8):1284-1293.
4. Keel P, Brown T. Update on course and outcome in eating disorders. Int J Eating Disord 2010;43(3), 195-204.
5. King's College London. A General Practitioner's guide to eating disorders; 2009 King's College London. www.iop.kcl.ac.uk
6. Pritts SD, Susman J. Diagnosis of eating disorders in primary care. American Family Physician. 2003;67(2):297-304.
7. NICE NG69. Eating disorders: recognition and treatment; 2017. https://www.nice.org.uk/guidance/ng69
8. Royal College of Psychiatrists. MARSIPAN: management of really sick patients with anorexia nervosa. College report CR162; 2010. https://www.rcpsych.ac.uk/docs/default-source/improving-care/better-mh-policy/college-reports/college-report-cr189.pdf?sfvrsn=6c2e7ada_2