Anxiety: assessment and management
Dr Mark Gillespie
Dr Mark Gillespie
RMN,BA(CPN),PGCert(TLHE), PGDip(PSI) Med
Nurse lecturer (mental health)/programme lead,
The University of the West of Scotland
General practice nurses are often the first healthcare professionals to encounter people experiencing anxiety and anxiety disorders: this article aims to support you in the identification, assessment, treatment and referral of such patients
Anxiety presentations are understood to be manifestations of the protective evolutionary mechanism known as the fight or flight response. This response incorporates a pattern of physiological, behavioural, emotional and cognitive changes that for most will be mild and time-limited and help manage or avoid the threats we associate with everyday life. For some, however, these changes will develop into a sustained and often distressing clinical condition.
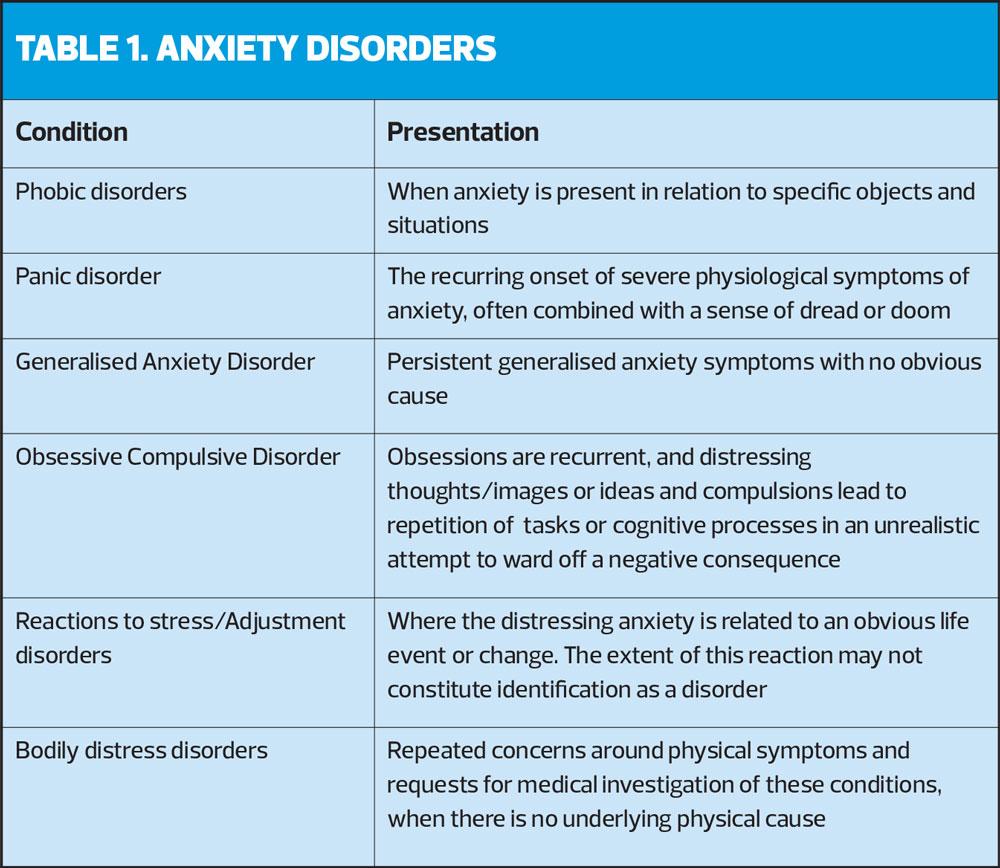
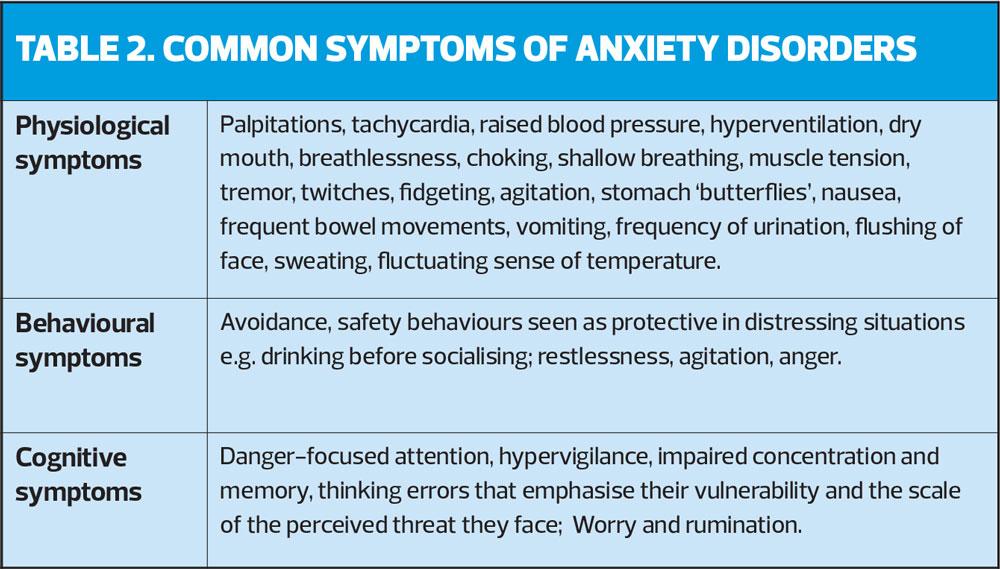
Six of the main forms of anxiety disorder as defined by the current International Classification of Disease1 are detailed in Table 1 while the more common symptoms of anxiety are identified in Table 2.
Many people are likely to experience anxiety symptoms over their lifetime, with around 3% of the population meeting clinical requirements for diagnosis at any one time,2 and around a third of the global population likely to present with anxiety symptoms across their lifespan. More females than males develop anxiety conditions and people being cared for by services managing physical and mental ill health are also at increased risk of developing anxiety as the condition co-exists with many other disorders. Primary care settings are an obvious access point for help with anxiety symptoms. Across the UK there are over eight million cases of anxiety diagnosed and in Scotland alone there are around half a million presentations to GP practices for this condition each year.3 General practice nurses play a vital role in providing an appropriate initial response, a role supported by current treatment guidance.
TREATMENT GUIDANCE AND THE STEPPED CARE APPROACH
In the UK there is clear direction around tailoring service response appropriately in relation to the severity of anxiety symptoms the individual is experiencing. This is set out in the NICE guidance on the management of Generalised Anxiety Disorder,4 and in Scotland in the NHS Education for Scotland (NES) document, ‘The Matrix’.5 There are several supplementary NICE guidelines on specific anxiety disorders, readily available on the NICE website. These clinical guidelines match patient need with treatment recommendations, and elevate response from the treatment of mild or transient anxiety by primary healthcare staff through to intense psychological therapies, such as Cognitive Behavioural Therapy, delivered by specialist practitioners, for more severe or enduring presentations. Across the UK there is a drive to link people suffering from anxiety (and depression) to appropriate psychological care without undue delay, generally within 18 weeks, and the primary care service is vital in meeting this target. Between 80% and 85% of contacts meet the target.
IDENTIFICATION AND ASSESSMENT OF ANXIETY SYMPTOMS
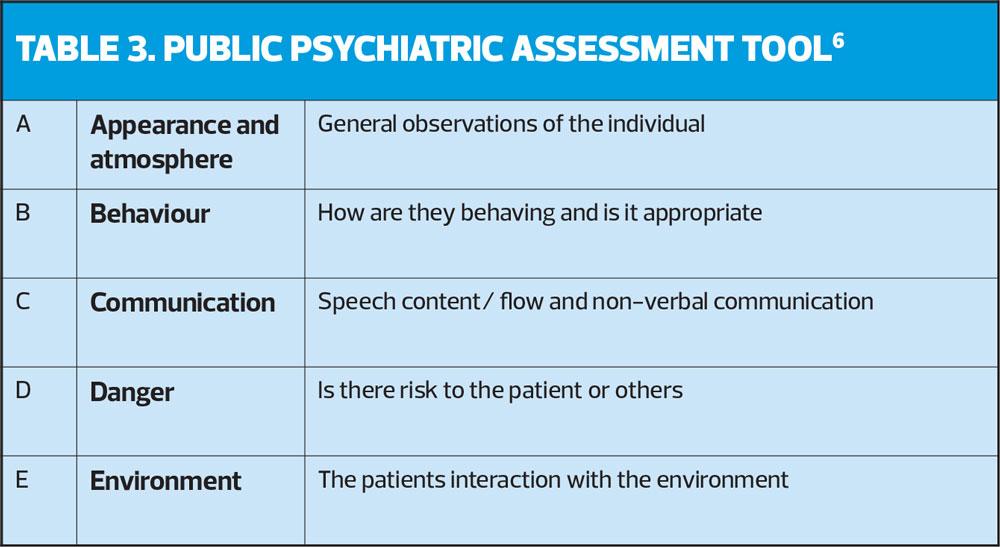
Early identification of any clinical disorder is beneficial as it can often aid the development of a collaborative nurse-patient relationship, reduce the duration of any distressing symptoms, initiate earlier treatment and lead to better outcomes for the individual patient. NICE has clearly identified a role for primary care practioners in screening for the presence of anxiety and in the initial assessment of the extent of symptoms.4 Screening for the presence of emotional distress or mental ill health should be a routine component of your patient interaction, and the Public Psychiatric Assessment Tool (PPAT) is a useful A-E framework that helps guide mental health assessment for professionals who are not mental health specialists.6 The PPAT was designed by staff from the University of Central Lancashire to help police officers assess for the presence of mental ill health in emergency situations,6 though it has now been adopted by several professional groups including paramedics, and is used across a wider range of situations. The PPAT is outlined in Table 3, though a more detailed explanation can be accessed via the original article.
If concerns are raised within the initial consultation any patient suspected of experiencing anxiety should be asked the first two questions from the Generalized Anxiety Disorder, seven question assessment tool, GAD-7.7 These questions are:
1. Over the last 2 weeks how often have you been bothered by feeling nervous, anxious or on edge?
2. Over the same timeframe how often have you been bothered by not being able to stop or control worrying?
There are 4 possible answers to each question and each answer has a score attached:
- Not at all – 0
- Several days – 1
- More than half the days –2, and
- Nearly every day – 3.
If the patient scores more than 3, a more thorough assessment is required and should be completed by a competent practitioner. As well as formats designed to identify generic anxiety and depressive symptoms such as the Hospital Anxiety and Depression Scale (HADS),8 there are several condition specific tools available, including completion of the entire GAD-7. The results of the assessments should then guide treatment or signposting the patient to the most appropriate service.
THE PRACTICE NURSE’S ROLE IN THE TREATMENT OF ANXIETY
Psychoeducation
As with working alongside any other patient, the development of a therapeutic relationship underpins the nursing care delivered. Using Carl Rogers’ core conditions of warmth, empathy, genuineness and unconditional positive regard9 will assist this. In this case normalising the person’s experience, demonstrating a level of expertise and interest and showing acceptance of the person’s situation will likely alleviate some of their fears and encourage them to engage with the assessment and treatment process.
Recovery for the patient often begins through understanding the nature of the condition they are experiencing and practice nurses should be able to deliver tailored packages of education, or psychoeducation as it is termed, as part of the initial management of the condition. Psychoeducation and symptom monitoring are identified as the immediate form of management for new presentations of mild anxiety and practice nurses are in a position to offer both. For patients that are acutely anxious or who have chronic, low level anxiety presentations there are a number immediate coping strategies and supports that can help alleviate the immediate crisis and build resilience around managing ongoing anxiety and preventing future exacerbations. Some of these approaches are outlined below and may be useful interim interventions for clients people with more severe presentations who require referral on to psychological treatment services.
Rodrigues et al’s recent meta-analysis10 identified that condition-related education in the treatment of anxiety was well accepted by patients, led to reductions in the severity of anxiety symptoms, worry and depressive symptoms and found that these improvements were sustained after the sessions had ended. These improvements were more likely to happen if a cognitive-behavioural method of education was used and this is the approach suggested here.
Patients and relatives will already have ideas and beliefs around what the patient is suffering from, how it should be treated, whether they think anxiety is the current problem and what anxiety actually means to them. Before commencing the delivery of any educational package it is important, therefore, to identify their current level of knowledge and understanding. This can be done by asking simple questions, such as ‘What do you think is causing this problem? What makes it better/worse? How should it be treated?’ This gives a baseline from which to gauge knowledge growth and also points out any strengths or gaps in their understanding.
There are several formats through which psychoeducation can be delivered and these should be considered in relation to the individual patient’s presentation and capabilities, and the range of options available. Initial consideration should identify whether one-to-one sessions were would be appropriate, or if a group setting would offer advantages, particularly around exposure and practice, both useful for people experiencing social anxiety. The inclusion of relatives also needs to be reviewed and some thought given to whether professional-led sessions would be more beneficial than peer led ones.
The cognitive-behavioural approach entails experiential learning whereby the patient is encouraged to actively consider the impact of anxiety as it relates to them. This requires them to investigate, identify and practise anxiety management techniques, supported through information, demonstration and feedback from others. There are choices available here around the media used to support this learning, with a variety of books, leaflets and online resources all available. Consideration should be given here to the patient’s literacy level, language capabilities and online access.
The content of educational sessions should include a normalising focus where the emphasis is on explaining the presentation as a more severe experience of the normal human response to stress. Physiological, cognitive and behavioural changes should all be explained in relation to anxiety and the effectiveness of treatment emphasised. Patients should be asked to identify current stressors and recent triggers and encouraged to consider their previous coping strategies for managing stress. The sessions should also involve information and practice on anxiety management techniques, forms of which are detailed below.
Online resources
Several effective online sources are available to support recovery from anxiety and patients experiencing mild anxiety or acute stress reactions can be directed to them for additional information and to commence low intensity psychological treatment. Moodzone11 is an NHS hosted website aimed at patients and provides useful information around stress, anxiety and depression. This site also includes relaxation tips and information on more intensive treatments available. Moodjuice12 is an NES website that offers access to separate resources for patients, carers and healthcare professionals. This includes information on managing common stressors and workbooks that the patient can complete.
Please remember that healthcare professionals also experience anxiety and that the online supports are useful for helping manage the stresses of clinical practice. Nurses should therefore consider using online resources alongside more formal support measures such as clinical and peer supervision to help develop their own resilience.
MEDICATION MANAGEMENT
Treatment guidance suggests that pharmacological measures should only be used where the patient’s anxiety is significantly impeding their daily functioning or when low intensity psychological approaches have not been effective.4 While Fry13 provides a more comprehensive consideration of the use of medicines, the most commonly used include anxiolytics, antidepressants and beta-blockers. Practice nurses should be fully aware of the common side effects, discontinuation symptoms and cautions that surround each of these medicines, and be actively involved in side effect monitoring around each.
STRESS MANAGEMENT TECHNIQUES
In addition to the delivery of psychoeducation there are a number of other techniques available to support the individual who is presenting with anxiety symptoms. For patients complaining of difficulty with sleep the use of sleep hygiene techniques such as caffeine reduction, preparation of a conducive sleep environment and avoidance of daytime napping are all helpful. To manage the anxiety symptoms, including worry, the use of deep breathing techniques, problem-solving training, Progressive Muscle Relaxation and Mindfulness should all be considered. These are all interventions that can be easily learned by both practitioner and patient, and be delivered within a brief consultation. In addition to these evidence-based interventions there are lifestyle changes that may also contribute to a reduction in anxiety experienced. These may include yoga, increased physical exercise and evaluation of lifestyle.
SUMMARY
Anxiety is a commonly occurring condition that will be impacting on many of the patients that you see. Practice nurses have a key role in screening for the presence of this disorder, and in the assessment, management and ongoing treatment of individuals experiencing anxiety symptoms. The more familiar you are with the current treatment guidelines and the supports available to you and your patients, the more effective you will be in helping reduce the distress those patients experience.
REFERENCES
1. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 11th Revision 2018. https://icd.who.int/browse11/l-m/en
2. Muir-Cochrane E, O’Kane D, Harrison. The person who experiences anxiety. In: Chambers (Ed) Psychiatric and mental health nursing; the craft of caring (Third edition) Abingdon. Routledge 2017. 215-224.
3. Information Services Division (Scotland). Anxiety, 2013. https://www.isdscotland.org/Health-Topics/General-Practice/GP-Consultations/Health-Conditions/Anxiety/
4. NICE CG113. Generalised anxiety disorder and panic disorder in adults; management, 2011. https://www.nice.org.uk/guidance/cg113
5. NHS Education for Scotland. A guide to delivering evidence based psychological therapies in Scotland, 2015 https://www.nes.scot.nhs.uk/education-and-training/by-discipline/psychology/the-matrix-(2015)-a-guide-to-delivering-evidence-based-psychological-therapies-in-scotland/the-matrix-(2015)-a-guide-to-delivering-evidence-based-psychological-therapies-in-scotland.aspx
6. Wright K, Glenn I, Dykes. Mental health emergencies: using a structured assessment framework. Emergency Nurse 2012;19(10):28-35
7. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine 2006;166(10): 1092-7.
8. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatry Scandinavia 1983;67:361-370.
9. Rogers RC. The necessary and sufficient conditions of therapeutic personality change, J Consulting Psychiatry 1957;21:95-103
10. Rodrigues F, Bartolo A, Pacheco, et al. Psycho-education for anxiety disorders in adults: a systematic review of its effectiveness. Journal of Forensic Psychology 2018. https://pdfs.semanticscholar.org/f0fe/fe1de07533843bdf2c516fe43987badfae50.pdf DOI: 10.4172/2475-319X.1000142
11. NHS. Moodzone 2017. https://www.nhs.uk/conditions/stress-anxiety-depression/
12. NHS Education for Scotland. Moodjuice https://www.moodjuice.scot.nhs.uk/mildmoderate/entry.asp
13. Fry M. Integrated therapy for anxiety. Practice Nurse 2012;42(10):28-31.
Related articles
View all Articles