Test results management in general practice: learning from clinical negligence claims
DIANE BAYLIS
DIANE BAYLIS
MSc, RN.
Clinical Risk and Education Manager, Medical Protection.
The way test results are handled in general practice is complex, and vulnerable to errors which can lead to patient harm and claims against the practice
The test result management system in general practice involves many members in the practice team, and there can be significant potential for system failure. An analysis of general practice claims over three years reveals some of the common issues contributing to patient safety incidents related to test result management. This article sets out tips to implement a robust test result system and highlights the importance of communication in this process.
Pressures on general practice are compounded by the fact that the work is becoming more complex and more intense.1 Therefore, it is not surprising that sometimes things go wrong. Errors can result in serious delays in treatment and harm to patients. In particular, inadequate follow-up after test results, and missed results, are more likely to have a greater impact on patients whose test results indicate the need for urgent treatment. Thus, it is vital that general practice teams have an understanding of the strengths and weaknesses in their test result system.
ANALYSIS OF CLINICAL NEGLIGENCE CASES
A Medical Protection study of 50 randomly selected claims from general practices over a three-year period – January 2014 to December 2016 – found that there was evidence of suboptimal management of test results.
The cases were reviewed by looking specifically at the factors that appeared to contribute to the patient experiencing an adverse event across two domains:
1. High level system domain (practice system interactions)2
2. Contributory factors domain, by using a framework for patient safety incident investigation
1. PRACTICE SYSTEM INTERACTIONS
Each case was reviewed in order to identify errors that had occurred involving each of the four stages of the management of test results process, as follows:2
a. Pre-analytical stage (test ordering stage)
b. Specimen processing stage (specimen being sent to the lab)
c. Post-analytical test stage (test results review and action stage)
d. Communication outcome issue (communicating test results to the patient).
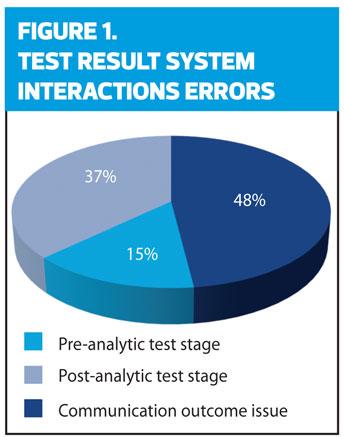
All but two of the 50 cases reviewed had one or more of the above systems interaction errors identified and 86% of the cases had two or more system errors. There were 85 system errors identified across the four stages. However, there were no errors identified in the specimen processing stage as shown in Figure 1.
SYSTEM INTERACTIONS CONTRIBUTING TO CLAIMS
a. Pre-analytic Test stage
Fifteen per cent of the system errors identified involved the Pre-analytic Test stage. These were errors about ordering a specific test:
- Failure to order the required test.
- Test not done as part of annual screening.
- Failure to follow-up or order blood tests requested by secondary care.
b. Specimen Processing stage
The specimens were successfully sent to the laboratory, and no errors were found at this stage. Incidents such as broken containers/package or lost specimens while in transit are possible errors in a different scenario.
c. Post-analytic Test stage
Thirty-seven per cent of the system errors identified involved the Post-analytic Test stage such as:
- Failure to forward the test result to the appropriate clinician.
- Lack of a ‘buddy system’ – if a GP is on leave, the practice administrator should assign the management of test results to another GP. Even if this is done, there may be delays.
- Not acting on results that require action.
- Result filed accidentally without being reviewed.
- Sub-optimal management of multiple results for a single patient – patient was informed that their test results were normal, when not all of their test results were back.
d. Communication outcome issue
Nearly half (48%) of the system errors were related to the communication of the test result, either between healthcare professionals, or doctor and patient. Similarly, a review of the reported incidents to the National Reporting and Learning System (NRLS) between October 2015 and September 2016 relating to test management, highlighted communication failure as a contributory factor in 31% of the reported incidents.3
Almost half (48%) of the 50 Medical Protection cases reviewed involved patient contact issues and failure to inform the patient of the abnormal test result. Often, it had been documented that the GP intended to advise the patient to make an appointment. But for various reasons, the GP did not convey this to the patient and therefore the abnormal result was not acted on. Such communication errors frequently resulted in a failure or delay to refer the patient for specialist treatment.
In addition, there were two cases involving a practice nurse who failed to notify the GP of an abnormal test result from a urine dipstick test which led to a delay in diagnosis of a serious medical condition.
2. CONTRIBUTORY FACTORS DOMAIN
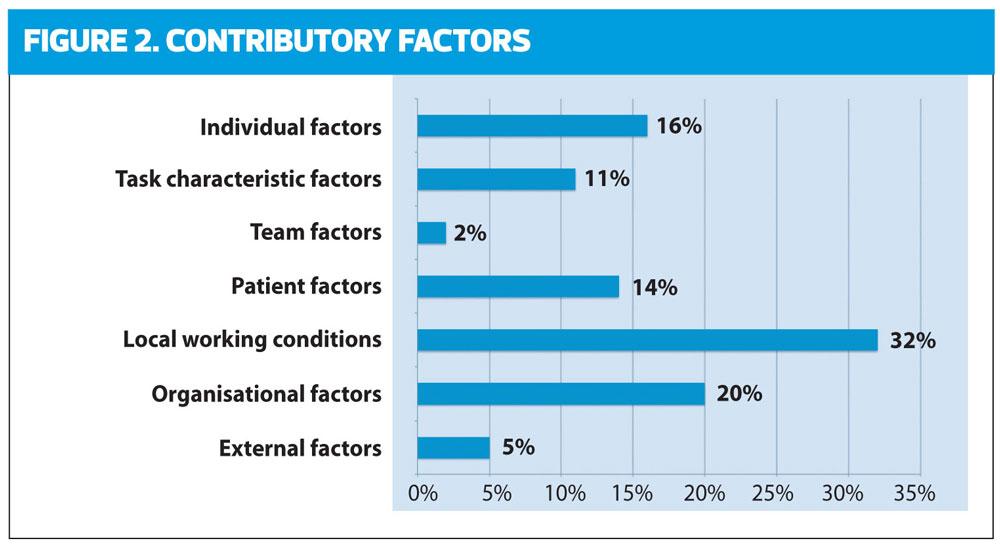
All 50 cases, in addition to system errors, had contributory factors, identified by using a framework for patient safety incident investigation known as the Yorkshire Contributory Factors Framework (YCFF).4 The framework uses the following parameters:
a. External factors
b. Organisational factors
c. Local working conditions
d. Patient factors
e. Team factors
f. Task characteristics
g. Individual factors
The YCFF tool aids our understanding at a system level of the interacting reasons why incidents may occur and enables practices to address identified system flaws more effectively.
Individual factors (16%)
- Inexperienced practice nurse who failed to undertake the blood tests requested by the GP, and misinformed the patient that their test results were normal.
- GP overlooked the abnormal test result by relying solely on the computer system.
- Locum GP may lack the knowledge of that particular practice’s system.
Task characteristic factors (11%)
- Data input error in computer system.
- Incorrectly picking the wrong drop-down box on the computer software. Thus, the patient was informed that their test was normal when they should have been directed to consult their GP.
- Complete reliance on the computer software to highlight abnormal results.
- Poor documentation.
Team factors (2%)
- Inappropriate task delegation.
Patient factors (14%)
- Patient did not fully understand the process because they had learning difficulties.
- Patient did not follow up with their test results.
- Patient with multiple medical conditions.
- Patient who frequently failed to attend appointments.
Local working conditions (32%)
- Unclear responsibilities for review or follow-up of test results.
- Lack of system to ensure test results are reviewed by the requesting clinician.
- Lack of continuity in patient care resulting in confusion over whose responsibility to ensure patient follow-up.
Organisational factors (20%)
- Lack of a consistent system to announce urgent action.
- Lack of practice systems for reviews or follow-ups; no annual recall system.
- Practice reliance on the patient to contact the practice for test results.
- Practice process of allocating the senior GP to review all the test results of patients whom they have not personally seen.
- No test result audit.
External factors (5%)
- Ambiguity about who was responsible for ordering a test, when the patient was under the care of both GP and the hospital.
- Ambiguity in referral guidelines for a specific condition.
- No clear system for sharing test results between primary and secondary care.
- Test results were sent to the wrong practice, in a shared building perhaps due to similar-named GP.
SUMMARY
Patients have expectations that their healthcare will be delivered to a high standard.5 Irrespective of the skill or dedication of the clinician, if the desired item of service is not actually undertaken or is delivered in a way that fails to deliver the expected result, patients can be at risk of harm.
There are many benefits from increasing reliability of the test results management system. Understanding the complexities of the interactions in the system contributes to a safer practice, in addition to a better use of time and resources. Hence, the expected care can be delivered more reliably.
Safe and reliable systems help to:
- Achieve consistent outcomes despite different individuals involved.
- Maintain standards.
- Reduce the likelihood and impact of individual error.
Practices can reduce test results errors if there is an open and learning culture where staff can freely raise potential safety risks. All staff should also be encouraged to take responsibility in identifying potential errors or weaknesses in the test results system.
Risks can also be reduced by ensuring regular reviews of the system of managing and reconciliation of test results, and having a system that tracks and reconciles tests requested against results received.
Inadequate or poor communication of test results to referrers and inadequate arrangements for a follow-up after the test results are nationally-acknowledged patient safety issues.6 Better communication between healthcare professionals and patients is vital to improve the test result system, thereby improving patient safety outcomes.
- Medical Protection’s Test Result 360, a user-friendly online tool, helps practices to develop a robust test result system. The tool takes about 15 minutes to complete, and it will provide a useful online audit of your test result system. To learn more or register: please visit www.medicalprotection.org/TR360, email crsa@medicalprotection.org or call 0113 241 0359.
CASE STUDY 1
EXAMPLE OF A TEST RESULT SYSTEM ERRORMr B, a 58-year-old, visited his GP with various health concerns. Dr G decided to undertake a series of blood tests, including a PSA (prostate specific antigen) test after discussing with Mr B.Mr B made an appointment to have the blood tests taken at the practice. He attended the appointment and had a number of samples taken by the practice nurse. However, she inadvertently failed to send a sample for the PSA test as requested.Mr B contacted the practice, as directed, to obtain his test results and was informed that they were all normal. He wrongly assumed that the PSA result was also normal. Dr G failed to notice that the PSA test was not included in the list of tests that he reviewed, as he relied on the computer system to ‘flag up’ any abnormal results.Mr B did not return to see Dr G for 12 months. Dr G then discovered that the PSA test had not been done previously and was very concerned about the patient and made an urgent specialist referral due to the severity of his symptoms. Unfortunately, Mr B was diagnosed with prostate cancer.Mr B then decided to make a claim against Dr G for clinical negligence as he felt that the diagnosis of cancer was delayed leading to a more invasive treatment for the cancer, which could have been avoided had the diagnosis been made at an earlier stage.
CASE STUDY 2A 22 year-old lady attended a surgery and was seen by the Advanced Nurse Practitioner (ANP). The patient complained of thirst and weight loss; she was concerned as she had a family history of diabetes. The ANP ordered bloods for fasting glucose.Two days later, the ANP reviewed the fasting glucose result and noted it to be 16.8mmols/The ANP documented that it was abnormal and sent an electronic message to the administration staff to recall the patient.The receptionist telephoned the patient to inform her that the ANP needed to discuss her test results and made an appointment for the patient to be seen in six days’ time. An appointment text reminder was sent.The patient failed to attend the appointment. The ANP telephoned the patient and it appeared that the patient had attended the wrong surgery (as the practice had two sites). The ANP advised the patient that the blood test needed to be repeated, followed by a consultation with the GP.The blood test was repeated and the result was significantly higher than the first test. Thus, the GP decided to make a home visit. However, the practice did not hold an up-to-date address of the patient – the GP went to the address of the patient’s parents instead and the patient was not seen.The patient attended a walk-in-centre the following day and was admitted into hospital.Key contributory factorsIndividual factorsThe ANP did not recognise the urgency of the raised glucose and did not ensure that the patient was given an urgent appointment with the GP.Patient factorsThe patient had not informed the practice of a change in her address.The patient attended the wrong site for her appointment.Organisational factorsThe practice has two sites. This may have confused the patient. The practice did not have systems to ensure that patient demographic details are kept up-to-date. This could easily be done if the patients are being asked about their contact details at various points of contact such as at the reception, during the consultation and through communication materials like a leaflet.
TOP TIPS FOR SAFER TEST RESULTS MANAGEMENTProtocolsRobust and standardised practice protocols can provide strong barriers against risks in the system that can protect against adverse events and avoidable harm to patients. They need to be designed by everyone involved in the work (including administration staff) and should reflect the local context of how the work is actually carried out and by whom, rather than being a high level and well-meaning guide which reflects an ideal rather than the everyday reality.1. The practice should operate a systems-based approach outlined in a formal written test result management protocol.2. The practice should undertake regular audits of the system to establish ongoing reconciliation performance at four stages – Pre-analytical (test ordering), Specimen processing, Post-analytical and Communication outcome.3. The practice should be fully aware that they are solely accountable for the management and communication of test results to patients that are undertaken within the practice.TrainingCommitment to training and raising awareness of roles can provide strong barriers against risks in the system to protect against adverse events and avoidable harm to patients.1. All clinical and administrative staff should be trained in applying those steps and tasks outlined in the protocol that are relevant to their job role and responsibility.2. All non-clinical staff members dealing with results must have appropriate training in the test result process.3. New staff and locum GPs should be provided with a written protocol outlining the practice system for test ordering and results management as part of induction.
REFERENCES
1. The Kings Fund, Understanding pressures in general practice, 2016
2. Bowie B, Price J et al, System hazards in managing laboratory test requests and results in primary care: medical protection database analysis and conceptual model. BMJ Open December 2015 http://bmjopen.bmj.com/content/5/11/e008968
3. NHS Improvement, Organisation patient safety incident reports (September 2016):
https://improvement.nhs.uk/resources/organisation-patient-safety-incident-reports-28-september-2016)
4. Improvement Academy. A Framework for Patient Safety Incident Investigation: Yorkshire Contributory Factors Framework (YCFF)
5. Bowling A, Rowe G, and McKee M. Patients’ experiences of their healthcare in relation to their expectations and satisfaction: a population survey. Journal of the Royal Society of Medicine 2013 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3618164/
6. Bowie P, Forrest E, Price J, et al, Good practice statements on safe laboratory testing: A mixed methods study by the LINNEAUS collaboration on patient safety in primary care. European Journal of General Practice 2015
http://www.tandfonline.com/doi/pdf/10.3109/13814788.2015.1043724?needAccess=true