Bracing ourselves for the annual flu season
MANDY GALLOWAY
MANDY GALLOWAY
Medical writer,
Editor, Practice Nurse
With experts predicting that ‘Aussie flu’ – which has caused the ‘worst flu outbreak in recent years’ – is heading for our shores, it is vital that as many eligible people as possible are vaccinated as possible
By now the annual flu campaign is in full swing, and general practice nurses are up to their eyes in back-to-back clinics. In some practices, GPNs are being given only 2 or 3 minutes per patient, and in one case Practice Nurse came across, the time allocated to check the patient’s details, eligibility, suitability for vaccination, administration and recording was just 1 minute. Superwoman, eat your heart out!
With all the rush, it is easy to get confused by who should receive which vaccine and when, and by the details of the at risk groups.
So this update aims to pull together the guidance from various sources, and to offer an aide memoire for the clinical risk groups and targets for the 2017-18 campaign.
So these are the eligible groups this winter:1
- All children aged 2 to 8 years (but not 9 years or older)
- All primary school children
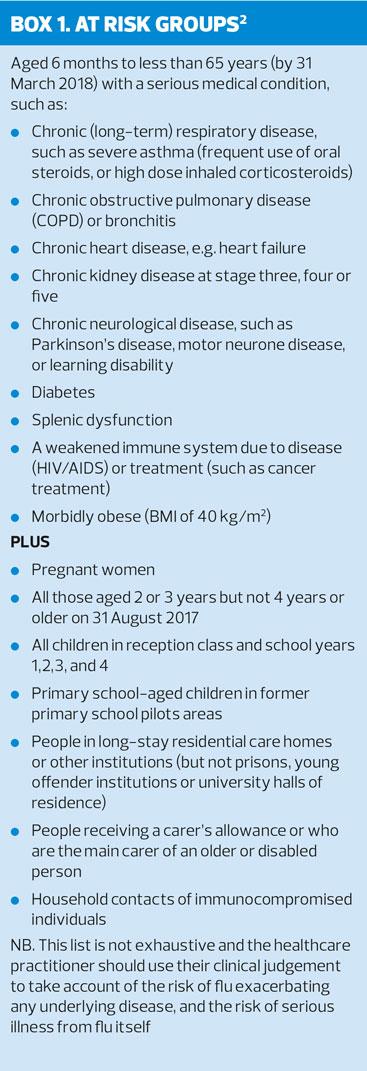
- All those aged 6 months to under 65 years in clinical risk groups, including those who are morbidly obese
- Pregnant women
- Those aged 65 years and over
- Those in long-stay residential care homes
- Carers
- Frontline health and social care workers. (Vaccination should be provided by their employer). (See also Box 1)
The key change to the children’s flu vaccination programme is that this year children aged 4 (as of 31 August 2017) to 5 years should be vaccinated at school, and not in general practice unless they are also in an at risk group. In other cases, the practice will be unable to claim payment under the DES (Direct Enhanced Service). Children aged 2 (on 31 August 2017) and 3 years will continue to be vaccinated in general practice.2
Controversially, flu vaccination will continue to be available through community pharmacies this season.
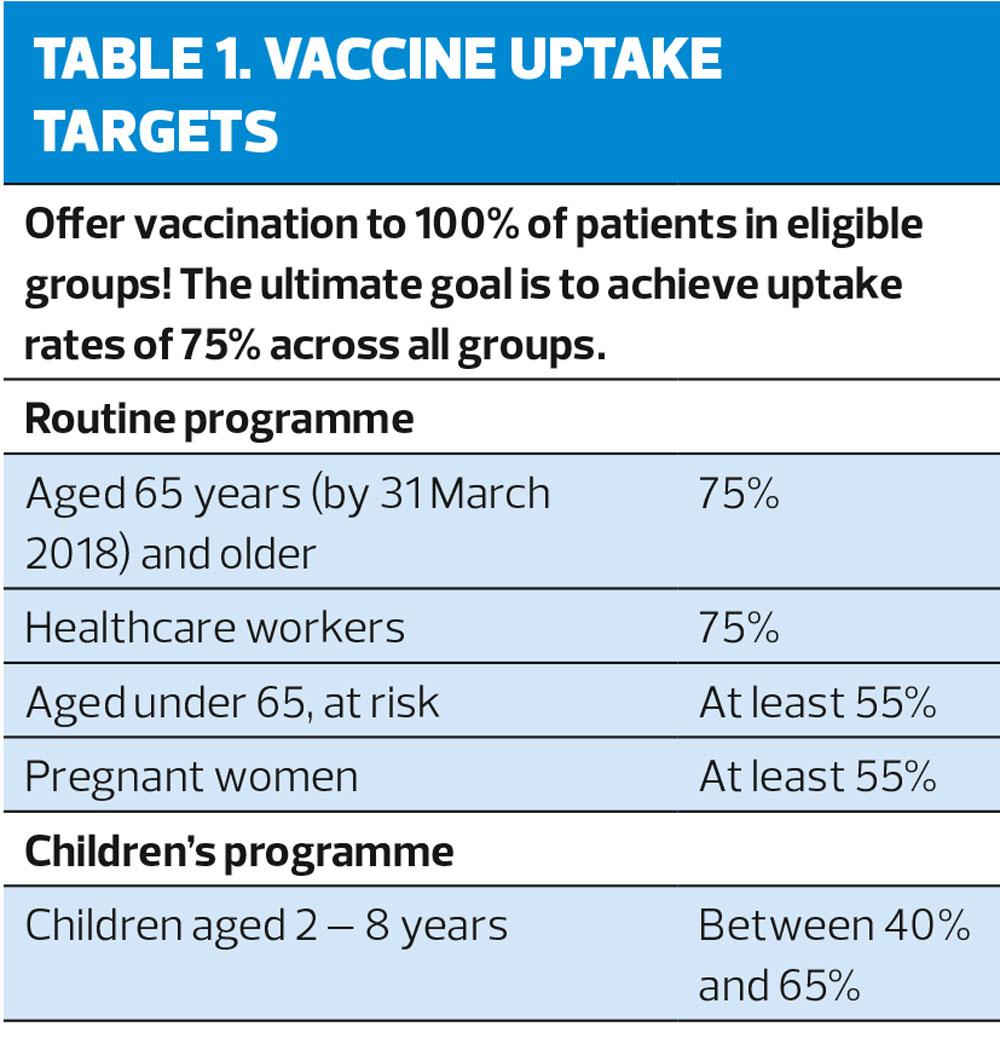
The uptake targets are shown in Table 1. Practices have been urged to redouble their efforts to improve uptake for those in clinical risk groups, particularly for those who are at the highest risk of mortality but who have the lowest rates of vaccine uptake.1
Vaccine uptake is particularly low in children under 16 years with clinical conditions that put them at most risk of complications or hospitalisation from flu, notably those with neurological disease including learning disabilities.
Pregnant women are particularly vulnerable to severe complications of flu. Between 2009 and 2012, 1 in 11 maternal deaths was due to flu infection. Ideally, they should be offered vaccination by their midwife, but this may not always happen, and practices are urged to ensure that women who become pregnant during the flu season are encouraged to have the vaccination.2
Among the clinical risk groups, those who are at greatest relative risk (RR) of death from flu are patients with chronic liver disease (RR = 32.8% – 70.6%), immunosuppression (RR = 35.1% - 63.1%) and chronic neurological disease, excluding stroke or transient ischaemic attack (RR = 28.7% – 56.8%). Conversely, the group that you might have thought to be at greatest risk, those which chronic respiratory disease, have a relative risk of only 5.5% – 10.0%.2
PHE says: ‘Despite continued efforts, for a number of years only half of patients in clinical risk groups have been vaccinated. For 2017-18, the ambition for this [group] is to achieve at least 55% uptake.’ Uptake in those with diabetes is already higher than 55%, but ultimately the goal is to achieve 75% across all the at risk groups.2
INFLUENZA
Flu occurs ever winter in the UK and is a key factor in NHS winter pressures. It impacts both on those who become ill and the NHS services that provide care. The annual flu campaign aims to reduce the impact of flu. The children’s flu programme is being extended to all children in a phased roll-out, because this has been shown to reduce transmission across the population, and indirectly, to protect older and more vulnerable people. So far, the vaccination of children has been shown to reduce the number of GP attendances for flu-like illnesses, and emergency department attendances for respiratory illness across all age groups.
Vaccines are produced each year to provide protection against the three strains of flu that the World Health Organization considers may be most prevalent the following winter. Flu viruses are constantly circling the globe, and generally speaking, the strains that are prevalent in the Southern Hemisphere in winter (our summer months) will be those that will reach us the next winter.
During their circumnavigation, viruses can mutate, and this can affect the efficacy of the vaccine. In recent years, vaccine has typically been around 50% effective – but this has ranged from 25% to 75%. In 2014-15, antigenic drift (the process by which the flu virus strains mutate) in the A(H3N2) strain meant that this component of the vaccine did not provide much protection.
Despite concerns about potential lack of effectiveness, PHE insists the vaccine remains ‘our best defence’ against flu.1
The impact of flu on the population varies from year to year, depending on the viruses that are in circulation. Over the past 50 years, there have been four serious flu epidemics, the most recent in 1989-90 when more than 600 per 100,000 population reported flu or flu like illnesses.2
The virus strains that are included in the 2017-18 season are:2
- An A/Michigan/45/2015 (H1N1)pdm09-like virus
- An A/Hong Kong/4801/2014 (H3N2)-like virus
- A B/Brisbane/60/2008-like virus2
In addition, quadrivalent vaccines will contain a second B-virus – B/Phuket.3073/2013-like virus.2
It is considered that the A-strains cause most cases of serious illness, and where the strain identified in a flu-like illness is one of the B-strains, it is not always possible to identify which particular strain is involved. However, B-strains can contribute to higher numbers of less severe illness.3
AUSTRALIA
Australia is experiencing its worst flu season for several years, with nearly 94,000 laboratory-confirmed cases reported to its National Notifiable Diseases Surveillance System by mid-August, and at least 170,000 cases by the end of September.3
The number of cases is 2.5 times higher than in the same period last year, and visits to GPs and hospital admissions are up 50% on last year. The groups that seem to be most at risk are the elderly (over 80 years) and children between the ages of 5 and 9 years.
So far, more than 50 deaths have been reported in Australia this year, although officials say that there is no evidence that the virus is causing particularly severe infection – just that the number of cases is much higher than in recent years.
The strains involved in the outbreak are predominantly Influenza A (H3N2), which has caused the majority of the deaths, but also some B strains, which tend to cause greater numbers of less severe infections.
Australia’s Department of Health has stated that the outbreak appears now to be waning, and that ‘the seasonal influenza vaccines appear to be a moderate to good match for circulating virus strains’ – but that effectiveness estimates will only become available towards the end of the season.3
US experts are predicting that the Australian epidemic ‘bodes ill’ for countries in the Northern Hemisphere, where flu circulates later in the year. ‘In general, we get in our season what the Southern Hemisphere got in the season immediately preceding us,’ said Dr Anthony Fauci, director of the US National Institute of Allergy and Infectious diseases. ‘An intelligent guess, therefore, is that the north will probably have a bad flu season.’
Professor Robert Dingwall, professor of public health at Nottingham Trent University said: ‘It is almost inevitable that this will come to us. This wiil be potentially the worst winter [for flu] since the Hong Kong outbreak of 1968.’
WHAT’S NEW
Two new flu vaccines are either already available, or will be in time for the 2018-19 flu season.
Quadrivalent influenza vaccine (QIV) (split virion, inactivated) contains two A-strains and two B-strains (B/Victoria and B/Yamagata), whereas conventional vaccines only contain one B-strain. In 2015-16, of the reported cases of influenza B in Europe, 92% were in the B/Victoria group, which was not included in the WHO recommendations for the trivalent vaccine that year.4
It is claimed that the quadrivalent vaccines can counter the effects of mismatched vaccines and circulating flu strains, providing broader protection. It has been estimated that approximately 227,790 cases of flu could have been avoided over the past decade if the QIV had been in use.
QIV is available in the UK for this season, and some practices have received QIV in their vaccine deliveries. It is licensed for use in adults and children from 3 years, and is listed as a vaccine available to order in the CMOs’ annual flu letter.1
Fluad® is the first adjuvant trivalent influenza vaccine (aTIV) in the UK, and has been developed specifically to address the burden of flu in the over-65s.5
The Joint Committee on Vaccination and Immunisation (JCVI) has acknowledged that in published studies, aTIV offers higher immunogenicity and effectiveness in comparison with non-adjuvanted vaccines, and says that it could be introduced for the 2018-19 season.
The new vaccine is designed to provide a greater immune response in older people, whose ageing immune systems do not react as well as those in younger people, a process known as immunosenescence. The adjuvanted vaccine boosts the immune response, providing greater protection in the over-65s who are at greater risk of hospitalisation and substantial excess mortality than younger people.
Although only just launched in the UK, Fluad is already in use in other parts of Europe, the US and Canada. It has a good track record for effectiveness and safety, although in clinical trials, a higher percentage of those who were given aTIV reported mild to moderate, short-lived local and systemic reactions than in those receiving conventional trivalent vaccine.
REMINDER
Flu vaccine, whether inactivated or the live attenuated version, can be given at the same time as other live or inactivated vaccines. The Green Book says that there is no need to leave a 4-week interval between LAIV and other live vaccines, and if intramuscular and intradermal vaccines are given together, they should be administered at separate sites, and preferably in a different limb.6
REFERENCES
1. NHS England. CMOs’ annual flu letter, 2017. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600880/annual_flu__letter_2017to2018.pdf
2. Public Health England/Department of Health/NHS England. Flu Plan Winter 2017/18.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/600532/annual_flu_plan_2017to2018.pdf
3. Australian Government Department of Health. Australian Surveillance Report and Activity Updates Report No 09, 2 September to 15 September 2017. http://www.health.gov.au/flureport
4. Sanofi Pasteur. Quadrivalent influenza vaccine now available for the 2017-18 influenza season (press release), September 2017. http://www.sanofi.co.uk/l/gb/en/layout.jsp?cnt=0114CCE6-D87F-45E9-8DFC-054E83F6A284
5. Seqirus. New influenza vaccine offers improved protection for older adults (press release), August 2017. http://www.seqirus.com/newsroom/New-influenza-vaccine-offers-improved-protection-for-older-adults
6. Public Health England. Immunisation against infectious diseases (the Green Book). Chapter 19, Influenza https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/456568/2904394_Green_Book_Chapter_19_v10_0.pdf