Stepping away from inertia in diabetes care
BEVERLEY BOSTOCK COX,
BEVERLEY BOSTOCK COX,
RGN, MSc, MA, QN
Nurse Practitioner Mann Cottage Surgery Moreton in Marsh
Education Lead, Education for Health Warwick
‘Clinical inertia’ explains why we do not always do all that we could in terms of delivering optimum care, but if we could avoid inertia in lifestyle change, glycaemic control, blood pressure and lipid management, the impact on outcomes in diabetes could be significant
Diabetes is a condition with many targets. A respiratory colleague mentioned to me recently that ‘diabetes is easy because you just have to hit those numbers’. Would that it were quite that easy! Deciding which numbers to aim for, reminding ourselves and the people we are treating why we are aiming for them and then deciding the best way to aim for them are just some of the skills required to optimise outcomes in this multi-faceted condition.
The NICE guideline on the management of type 2 diabetes1 respects the clinician’s ability to choose the most appropriate targets and drug management for each individual. The newly published guidelines from SIGN are similarly set out to ensure that clinicians recognise the variety of options available.2 There are broad recommendations but a breadth of choices and options, which should enable clinicians and people with diabetes to make the most appropriate selection from a list of drugs aimed at improving outcomes. Specifically, as diabetes is a cardiovascular disease, reducing cardiovascular risk is at the heart of many choices that are made. The key complications of diabetes are microvascular diseases such as nephropathy, neuropathy and retinopathy, which can be harbingers of the macrovascular complications: myocardial infarction, stroke and peripheral arterial disease.3 Therefore, lipid and blood pressure management are as crucial as glycaemic control and taking a robust approach to all three of these areas is likely to lead to fewer complications in the future.
The best way to manage diabetes is through a combination of lifestyle interventions and pharmacological therapies as each complements the other. If we can avoid inertia over lifestyle change, glycaemic control, blood pressure management ant lipids, the impact on outcomes in diabetes care could be significant. Here are four steps to reduce inertia in diabetes care:
AVOIDING INERTIA IN LIFESTYLE CHANGE
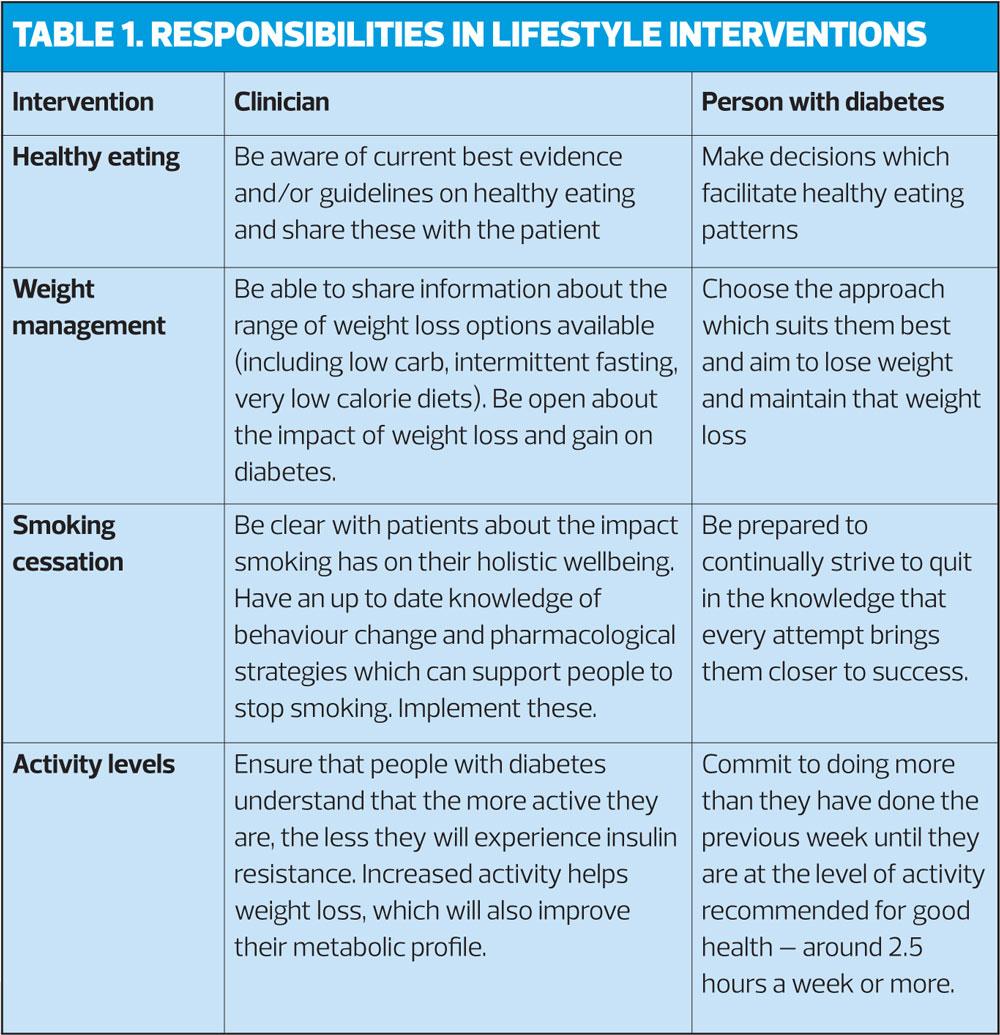
There is an increasing amount of discussion in the world of medicine and beyond, about the need to remember that many of the health issues facing us – in the western world in particular – could be significantly reduced by simply living a healthier lifestyle. Huge amounts of resources are ploughed into encouraging people to eat healthily, reduce their alcohol intake, increase activity levels and stop smoking. We have entire programmes and departments (the NHS Health Checks and Diabetes Prevention Programme, for example) dedicated to getting this very simple message out. It is absolutely essential that people with (or at risk of) diabetes (or cardiovascular disease, or cancer, or arthritis and so on and so on) realise that following the broad principles of a healthy lifestyle is their best insurance policy against these conditions and optimises their chances of reducing the associated risks if they have already been diagnosed. In the context of Making Every Contact Count, every opportunity should be taken to remind people that lifestyle changes can have a huge impact on current and future wellbeing and support people to make simple but important lifestyle changes.7 (Table 1, page 17) Motivational interviewing techniques and cognitive behavioural therapy can help people to move forward with making change happen.8,9
AVOIDING INERTIA IN GLYCAEMIC CONTROL
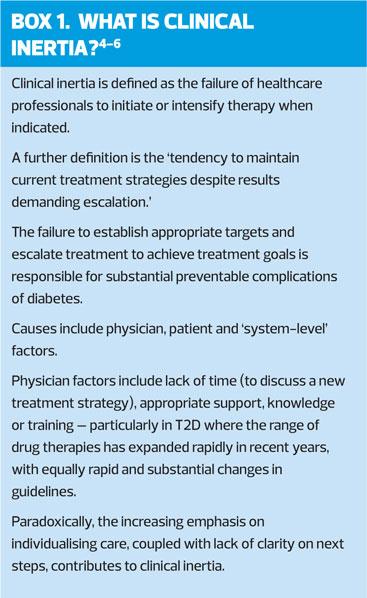
In diabetes management, the focus is often on glycaemic control with decisions being made based on the HbA1c and the individual’s own lifestyle, preferences and risk profile. NICE suggests aiming for a target of 48-58mmol/mol, with the actual target being decided upon by the patient with support from the clinician. Patient decision aids can also be used to help people to decide how best to control their blood glucose levels.10 With metformin being the first line choice for most individuals (weight neutral, possible small weight losses for some people, cardio-protective and no risk of hypoglycaemia) the decision making process really starts to happen at the first and second intensification of glucose lowering agents. The target HbA1c for someone who is only on metformin should be 48mmol/mol.1 Tight control early on, optimises outcomes – the so-called legacy effect11 – so failing to recognise this and act upon it by encouraging people to aim for this target could be deemed ‘clinical inertia’.12 Dictionary definitions of ‘inertia’ include words like apathy, idleness and stagnation, which do not sit well with evidence based practice. If targets (along with the rationale for those targets) are not shared with people who have diabetes they cannot make informed decisions about their management and this failure to inform breaches concepts such as autonomous decision making and informed consent.13
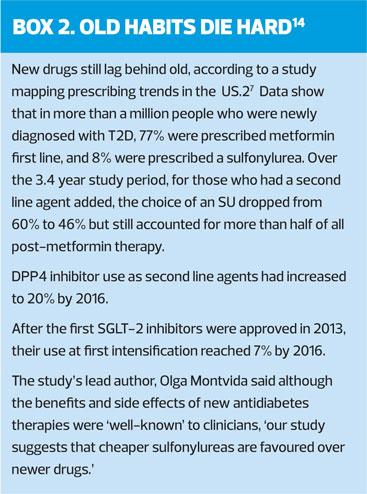
Once the HbA1c rises above 48mmol/mol with a combination of metformin and lifestyle interventions, another drug should be introduced. So how do we choose? In essence, most people (clinicians and patients) will be looking for a drug which has the most benefits and the least risks or side effects. Sulfonylureas and insulin are the most risky in terms of hypoglycaemia and weight gain but obviously if someone needs insulin, because their pancreas is simply not making enough, then it must be initiated. However, the indications for introducing a sulfonylurea (SU) are far fewer. While SUs are potentially useful in the newly diagnosed, symptomatic patient, they should be a short-term measure only because of their poor risk: benefit profile. In terms of steps 2 and 3 in glycaemic control, the main choices are the DPP4 inhibitors (the gliptins) and the SGLT2 inhibitors (the flozins).
In many patients, the first and second intensification will involve these two drug classes as they offer an attractive risk: benefit profile as shown in Table 2. None of these first three drug options requires routine home blood glucose testing either, which is good for the patient and has cost benefits.
If triple therapy has not worked then it might be time to consider whether drugs that are not having an effect should be withdrawn before introducing other options. GLP1 mimetics, such as Victoza, Trulicity or Bydureon, work on the incretin pathway, as do DPP4 inhibitors so these are not normally used together as their actions overlap.
The LEADER study15 recently reported some positive cardiovascular outcomes when using Victoza, which is a daily injection. Trulicity and Bydureon are weekly injections, which might be preferable for many individuals, and the results of further cardiovascular studies using once weekly GLP1s are anticipated soon.
Pioglitazone has its pros – it does not cause hypoglycaemia and can be used in renal impairment – but it also has its cons. The cons include weight gain, an increased risk of fractures and the ebb and flow of the bladder cancer signal. There is a place for pioglitazone but it needs to be chosen with care.
In general, however, if glycaemic control has not been achieved with three agents, it may be time to consider insulin. In a recent study on diabetes clusters, where five different cluster types of diabetes were suggested, severe insulin deficiency in people with non-autoimmune diabetes was recognised as an important sub-group.16 If people are insulin deficient, insulin replacement will be needed to control blood glucose levels. As we move from single therapy to dual therapy and triple therapy, targets are relaxed to 53mmol/mol and 58mmol/mol. However, it should be recognised that the higher the HbA1c, the greater the risk of long-term complications. The clinician should support people to understand this and to aim for the best control possible, but using drugs with the best risk: benefit profile in terms of hypos, weight gain and cardiovascular benefit.
AVOIDING INERTIA IN BLOOD PRESSURE MANAGEMENT
Many people with diabetes will also have hypertension. The suggested target for blood pressure is 140/80mmHg unless the individual has complications of their diabetes, in which case the target would be 130/80mmHg.1 The first line treatment for hypertension in people with diabetes is an ACE inhibitor or angiotensin receptor blocker (ARB), optimised to the maximum tolerated dose in order to maximise the cardioprotection and renoprotection that these drugs offer.17 It is well recognised, however, that people with hypertension often need at least two and maybe even three drugs to control their blood pressure, so other classes of drugs should be considered if good control is not achieved using just an ACE inhibitor or and ARB. The second drug would usually be a calcium channel blocker and the third drug would be indapamide.21 Treating hypertension reduces the risk of complications in the future as well as having a positive impact on the kidneys. This is why it is so important to manage blood pressure effectively. Again, this is something that should be shared with the patient so that they understand why we monitor and manage this risk factor, even though they may not feel any ill effects from a raised blood pressure.
AVOIDING INERTIA IN LIPID MANAGEMENT
Lipid lowering therapies have often been the victim of bad press, leaving people at risk if they decide not to take statins. Although autonomous decision making is essential in healthcare, people need to have access to reliable, evidence based sources of information in order to make their decisions. There is a wealth of evidence for the use of lipid lowering therapies in people with diabetes,22-24 and again, this should be shared. In primary prevention, where people do not already have a diagnosis of cardiovascular disease, statins are normally recommended in people who have a risk score (using QRisk) of 10% or more. If the score is over 10%, atorvastatin 20mg daily should be initiated with the aim of reducing non-HDL cholesterol to 2.5mmol/l.25 A non HDL cholesterol value of 2.5mmol/l equates to an LDL cholesterol value of 1.8mmol/l. If the non HDL cholesterol target of 2.5mmol/l is not achieved, the dose of atorvastatin can be uptitrated to 40mg or higher. There is also the option to introduce ezetimibe as a non-statin therapy which complements the action of the statin and which has been shown to reduce LDL cholesterol and improve cardiovascular outcomes.26 Statin side effects are dose-related so this can be a useful option for people who cannot reach target on lower doses of statins but cannot tolerate higher doses; an alternative approach would be to use higher intensity statins at lower doses such as rosuvastatin at 5mg. Effective lipid management should be achievable for most people with the right discussions and appropriately tailored therapy.
THE STATE OF THE NATION
Diabetes UK has been producing ‘State of the Nation’ reports on diabetes for a number of years, and many of them make for depressing reading. In the 2016 version, it was reported that the state of diabetes services in England was unduly unhealthy, with significant variations in care for people with diabetes and with too many people with diabetes not receiving the support they need to help them manage their condition and reduce their risk of ‘devastating and costly’ complications.27
There are many reasons why diabetes is poorly managed. Some will relate to different populations, some to clinicians, including their own level of knowledge and understanding of the evidence. However,
if clinicians and people with diabetes understand why the targets are in place and how we can work together to achieve them, we have a better chance of reducing the significant impact that diabetes has on the individual, the NHS and society in general.
REFERENCES
1. NICE NG28. Type 2 diabetes in adults management, 2015 (updated 2017) https://www.nice.org.uk/guidance/ng28
2. SIGN 154. Pharmacological management of glycaemic control in people with type 2 diabetes, 2017 http://www.sign.ac.uk/assets/sign154.pdf
3. Gaede P, Oellgaard J, Carstensen B, et al. Years of life gained by multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: 21 years follow-up on the Steno-2 randomised trial. Diabetologia 2016; 59(11):2298-307
4. Khunti S, Davies M, Khunti K. Clinical inertia in the management of type 2 diabetes mellitus: a focused literature review. Br J Diabetes Vasc Dis 2015;15:65-69
5. Strain WD, Cos X, Hirst M, et al. Clinical inertia in individualising care for diabetes: is there time to do more in type 2 diabetes. Diab Res Clin Pract; 2014:302-12
6. Strain WD, Blüher M, Paldánius P. Clinical inertia in individualising care for diabetes: is there time to do more in type 2 diabetes? Diabetes Ther 2014;5(2):347-354
7. Public Health England. Making every contact count, 2016. https://www.gov.uk/government/publications/making-every-contact-count-mecc-practical-resources
8. Rollnick S, Miller WR, Butler CC. Motivational Interviewing in Healthcare. New York; Guilford Press: 2008
9. David L. Using CBT in General Practice, second edition: The 10 Minute CBT Handbook. Oxfordshire; Scion Publishing: 2013
10. NICE NG28. Type 2 diabetes management: Patient decision aid, 2015 https://www.nice.org.uk/guidance/ng28/
resources/patient-decision-aid-1687717
11. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577-89
12. Khunti K, Wolden ML, Thorsted BL, et al. Clinical Inertia in People With Type 2 Diabetes. Diabetes Care 2013;36(11):3411-17 https://doi.org/10.2337/dc13-0331
13. Beauchamp TL, Childress JF. Principles of Biomedical Ethics Oxford; Oxford University Press:2013
14. Montvida O, Shaw J, Atherton JJ, et al. Long-term trends in antidiabetes drug usage in the US: real-world evidence in patients newly diagnosed with type 2 diabetes. Diabetes Care 2017; dc171414 http://care.diabetesjournals.org/content/early/2017/11/04/dc17-1414
15. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes N Engl J Med 2016;375:311-322
16. Ahlqvist E, Storm P, Karamajanaki A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables The Lancet 2018. DOI: https://doi.org/10.1016/S2213-8587(18)30051-2
17. Heart Outcomes Prevention Evaluations Study Investigators (2000). Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 2000;355:253-59.
18. Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015;373:232-242 http://www.nejm.org/doi/full/10.1056/NEJMoa1501352#t=article
19. Neal B, Perkovic V, Mahaffley KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabets. N Engl J Med 2017;377:644-657 http://www.nejm.org/doi/full/10.1056/NEJMoa1611925
20. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-2128 http://www.nejm.org/doi/full/10.1056/NEJMoa1504720
21. NICE CG127. Hypertension in adults: diagnosis and management, 2011 (updated 2016) https://www.nice.org.uk/guidance/cg127
22. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364: 685–96
23. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003;361:2005–16.
24. Sever PS, Dahlöf B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial—Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003;361:1149–58.
25. Joint British Societies’ Consensus recommendations for the prevention of cardiovascular disease (JBS3). Heart 2014;100:ii1-ii67 http://heart.bmj.com/content/100/Suppl_2/ii1
26. Cannon CP, Blazing MA, Giugliano RP, et al (2015) Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med 372:2387-2397
27. Diabetes UK. State of the Nation report, 2016 https://www.diabetes.org.uk/Global/get-involved/campaigns/Diabetes%20UK%20State%20of%20the%20Nation%202016.pdf