Managing type 2 diabetes – beyond glycaemic control
BEVERLEY BOSTOCK-COX
BEVERLEY BOSTOCK-COX
RGN MSc MA QN
Nurse Practitioner Mann Cottage Surgery, Moreton in Marsh
Education Lead Education for Health, Warwick
Recent studies of newer glucose-lowering therapies indicate that some may also help to protect against cardiovascular and other complications of diabetes, beyond simply lowering blood glucose levels. In this article we will consider the increasing body of evidence for an extended role for some of the agents used in the management of type 2 diabetes
Ask a member of the public what diabetes is and the first thing they are likely to mention is sugar. Ask a clinician how they manage diabetes and the chances are that the first thing they will mention is glycaemic control. However, it is often said that diabetes is a cardiovascular disease and as a result there is an increased awareness of the role of managing lipids and blood pressure too, mainly on the basis of the close link between diabetes and cardiovascular complications.1 People with type 2 diabetes (T2D) are at increased risk of macrovascular complications such as coronary heart disease (CHD), stroke and peripheral arterial disease (PAD) and they are also at higher risk of microvascular complications including nephropathy, neuropathy and retinopathy.2 Recent studies of newer therapies that improve glycaemic control have indicated the possibility that some of these therapies may help to reduce cardiovascular risk beyond simply lowering blood glucose levels. In this article we will consider the increasing body of evidence for the role of some glucose lowering therapies have in delivering protection against cardiovascular and renal complications which goes beyond glycaemic control.
By the end of this article you should be able to
- Recognise the glucose lowering drugs which have evidence of cardiovascular benefit
- Evaluate the evidence for these drugs
- Identify people who may benefit from these drugs
- Know how to initiate and titrate these drugs
- Identify the licenced indications for the drugs mentioned
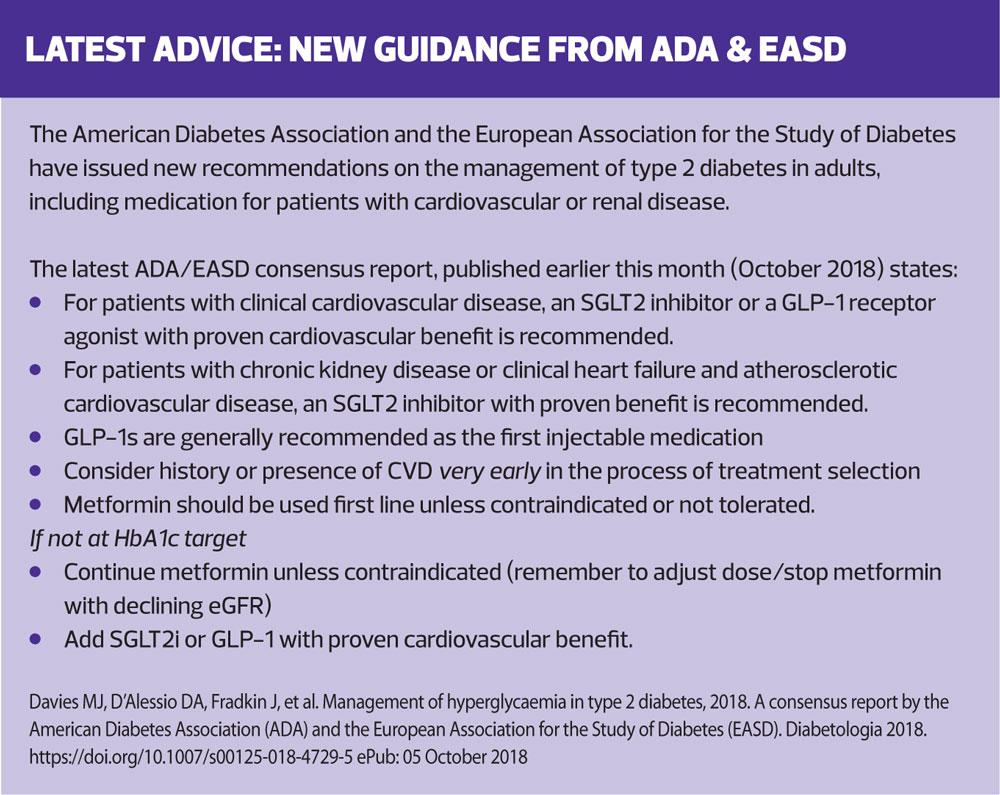
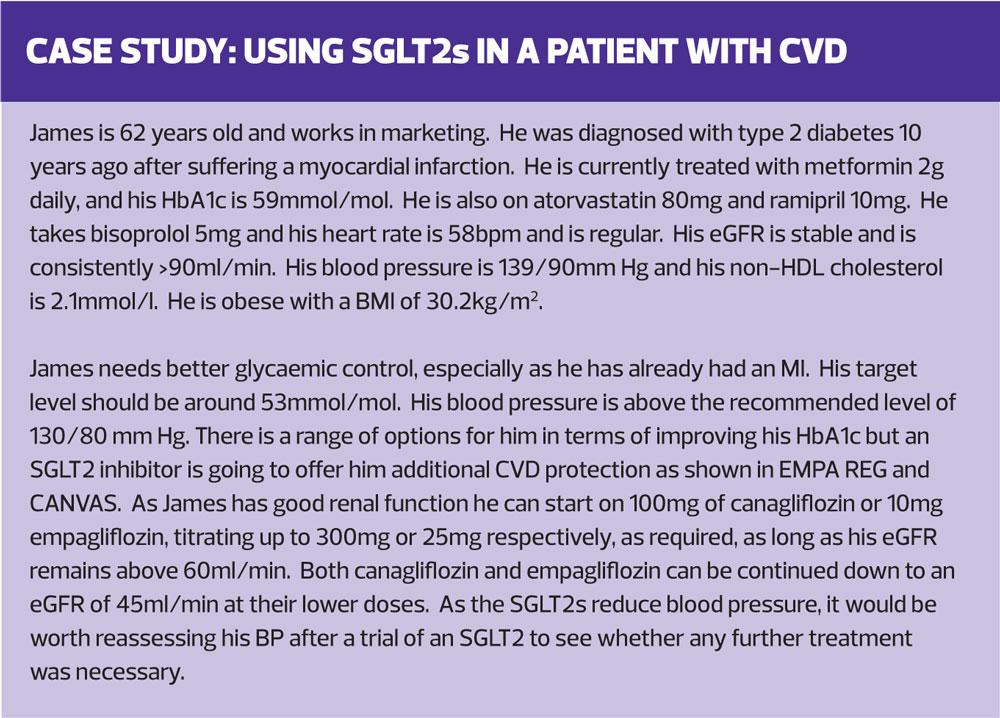
Diabetes has, for some time, been recognised as condition that has a high risk of causing cardiovascular complications.3 Thirty years ago, in 1998, Haffner et al published a paper which suggested that having diabetes led to the same risk equivalence of a future myocardial infarction as someone who had already had one.3 However, it is not just the heart that is affected by diabetes. End stage renal disease, leading to dialysis and significant mortality levels, is higher in people living with diabetes compared to those without diabetes.4 At a time when 10% of the total NHS budget is spent on diabetes, it is sobering to consider that most of that – around 80% in fact – is spent on treating the complications of the disease, not the disease itself.5 When there are pressures on the NHS to save money, it would appear that the greatest savings can be made by reducing complication rates, rather than through the prescribing budget. It is not surprising, then, that the recently published Scottish Intercollegiate Guidelines Network (SIGN) guideline on the management of T2D highlighted the importance of considering the use of the sodium-glucose cotransporter 2 (SGLT2) inhibitors canagliflozin and empagliflozin due to their proven cardiovascular benefits.6 These benefits were demonstrated in two ground-breaking trials examining the impact of these SGLT2 inhibitors. The Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG) study compared empagliflozin with placebo in patients with increased CVD risk.7 The Canagliflozin Cardiovascular Assessment Study (CANVAS) studied the impact of canagliflozin on individuals with T2D who were at high risk of, or with a history of, CVD.8 The results of the DECLARE study, which studied the impact of dapagliflozin on CVD risk, are due to be presented at the American Heart Association Scientific Sessions meeting next month (November 2018).9,10
EMPAGLIFLOZIN AND CARDIOVASCULAR BENEFITS
Over 7,000 patients were recruited to the EMPA-REG study, and they were followed up for an average of just over 3 years. The results were published in 2015.7 Patients who were eligible for the study had to be adults with a diagnosis of T2D and established cardiovascular disease and an estimated glomerular filtration rate (eGFR) of 30ml/min/1.73 m2 or more. Recruits had to have had no glucose-lowering therapies for at least 12 weeks before randomisation with an HbA1c of between 53mmol/mol and 75mmol/mol, or they had to have had stable glucose-lowering therapy for at least 12 weeks before randomisation with an HbA1c between 53mmol/mol and 86mmol/mol. All received standard care and were then randomised to empagliflozin 10mg, increasing to 25mg where indicated, or placebo. The primary outcome measured was death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke, comparing the empagliflozin-treated group with the placebo group. The primary outcome occurred in 490 of 4687 patients (10.5%) in the active treatment group and in 282 of 2333 patients (12.1%) in the placebo group (hazard ratio in the empagliflozin group, 0.86; 95.02% confidence interval, 0.74 to 0.99; P=0.04 [i.e. statistically significant] for superiority). In the empagliflozin group there were significantly lower rates of death from cardiovascular causes (3.7%, vs. 5.9% in the placebo group; 38% relative risk reduction), hospitalisation for heart failure (2.7% and 4.1%, respectively; 35% relative risk reduction), and death from any cause (5.7% and 8.3%, respectively; 32% relative risk reduction). In EMPA REG, it was shown that people with T2D at high risk for cardiovascular events who received empagliflozin, as compared with placebo, had a lower rate of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke and of death from any cause on this treatment when compared with those who did not receive the drug.
CANAGLIFLOZIN AND CARDIOVASCULAR BENEFITS
The Canagliflozin Cardiovascular Assessment Study – CANVAS - was published in 2017.8 This randomised controlled trial was designed to evaluate the impact of canagliflozin (100-300mg) versus placebo on the incidence of cardiovascular death, myocardial infarction, or stroke. The 10,142 patients included in the trial had to have a history of T2D and to be at increased risk of cardiovascular disease (CVD) with almost two thirds having a history of CVD. This is therefore a different study population than EMPA-REG as CANVAS included people at risk of CVD and not just people with established CVD, as was the case in EMPA-REG. Secondary prevention of CVD was examined by including people aged 30 years or more with a history of symptomatic atherosclerotic cardiovascular disease, whereas the impact on primary prevention was assessed through the inclusion of people age 50 or above with at least two risk factors for CVD, including having T2D for more than 10 years, (the average duration of diabetes was 13.5 years) having a systolic blood pressure of more than 140 mmHg on antihypertensive therapy, current smoking, the presence of albuminuria, or having a high-density lipoprotein (HDL) cholesterol of less than 1mmol/l. The average age of patients in the study was 63 and just over a third were women. CANVAS was a big study, with over 10,000 people enrolled into it and follow up was for over 3.5 years (188 weeks).
CANVAS demonstrated a statistically significant reduction in the primary outcome of incidence of cardiovascular death, myocardial infarction, or stroke, in the patients treated with canagliflozin, when compared with the placebo group.8 There were more events in the secondary prevention group than in the primary prevention group but the benefits of canagliflozin were seen across both groups.8 The benefit of canagliflozin appeared to be greater among people with a prior history of heart failure.8 This is an important finding and is discussed further below.
An additional benefit of SGLT2 inhibitors is their effect on blood pressure and lipid profiles. The blood pressure effect is thought to be the result of the reabsorption of sodium and glucose, leading to a mild osmotic diuretic effect and natriuresis leading to clinically significant reductions in both systolic and diastolic blood pressure.11 A systematic review and meta-analysis found that SGLT2 inhibitors appear to reduce systolic BP, by an average of 2.46 mm Hg and diastolic BP by an average of 1.46 mmHg.12 In addition, this analysis indicated that people being treated with an SGLT2 inhibitor had reductions in their total cholesterol and triglyceride levels.12
LEADER, LIRAGLUTIDE AND CARDIOVASCULAR BENEFITS
The Liraglutide and Cardiovascular Outcomes trial (LEADER) recruited 9,340 patients who were followed up for a median 3.8 years.13 These patients had T2D and were at high risk of a cardiovascular event. As with EMPA-REG and CANVAS, the primary composite outcome was the first occurrence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke. The event rate was significantly lower in the liraglutide group (608 of 4668 patients [13.0%]) than in the placebo group (694 of 4672 [14.9%]) (hazard ratio, 0.87; 95% confidence interval [CI], 0.78 to 0.97; P13 Of note is the fact that a similar trial looking at cardiovascular risk and once weekly exenatide did not show evidence of benefit, with the authors noting that among patients with T2D with or without previous cardiovascular disease, the incidence of major adverse cardiovascular events did not differ significantly between patients who received exenatide and those who received placebo.14
CANAGLIFLOZIN AND RENAL BENEFITS
In CANVAS,8 an acute reduction in eGFR was observed in patients treated with canagliflozin after 4 weeks of treatment, followed by stabilization in the rate of long-term decline in eGFR. This was similar to observations reported with empagliflozin in EMPA-REG.7 It is thought that this is an indication of altered renal haemodynamics and reduced intraglomerular pressure. Wanner11 has also described how the metabolic effects of T2D have a negative effect on the kidney through inflammatory cytokines, renal cell hypertrophy, and damage to the basement membrane. It had also been noted from the CANVAS study findings that there was evidence to suggest that there was a lower rate of progression of albuminuria in the active treatment group and that the cardiovascular benefits of canagliflozin were maintained irrespective of renal function.8 This led to further assessment of the impact of canagliflozin on renal function. The recent announcement that the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study has been ended ahead of schedule following positive results suggests that in future, drugs for diabetes control may also be selected on the basis of proven renal benefits.15
Recognising that around one third of people with T2D are at risk of renal impairment which can potentially lead to end stage kidney disease and which is also linked to an increased risk of CVD,16 CREDENCE examined the efficacy and safety of canagliflozin in people with T2D and chronic kidney disease (CKD). Study participants were on the maximum licensed and tolerated dose of an ACE inhibitor or an angiotensin 2 receptor antagonist for at least 4 weeks before the trial started. Key endpoints for the study included the time to dialysis or renal transplant and the time to doubling of serum creatinine and renal or cardiovascular death. There were 4,400 participants who were recruited with an eGFR between 30 and 89ml/min/1.73m2, and albuminuria (urinary albumin: creatinine ratio >300 to ≤5,000 mg/g) (>3mg/mmol to <50mg/mmol in UK measurements). The trial was halted early because of the evidence of benefit that was already being seen.15
Other SGLT2i's and evidence in renal impairment
As noted above, empagliflozin is already licensed for reducing cardiovascular death in patients with type 2 diabetes and CVD based on results from EMPA-REG but based on similarly positive findings in that trial, empagliflozin is also being trialled for CKD in people with and without diabetes.17 The findings are not yet available.
DIABETES AND HEART FAILURE
Studies have shown that people with T2D are at increased risk of developing heart failure.18,19 It is important, then, that any effect of diabetes management on heart failure risk or hospitalisation is minimised wherever possible. Pioglitazone is contraindicated in heart failure,20 and both saxagliptin and alogliptin have heart failure warnings assigned to them by the FDA.21 When it comes to the SGLT2 inhibitors, however, both canagliflozin and empagliflozin have shown a reduction in hospitalisations for heart failure in patients taking each SGLT2 inhibitor when compared with placebo.7,8 Empagliflozin showed a significantly lower risk of hospitalisation for heart failure in EMPA-REG,7 and canagliflozin showed the same advantage in CANVAS.8
ADDRESSING CONCERNS OVER LOWER LIMB AMPUTATIONS
CANVAS8 identified a very small but increased risk of lower limb amputations in canagliflozin users, but all SGLT2 inhibitors have warnings in their summary of product characteristics about this risk.22 However, a mechanism for this increased risk has not been identified (although it may be due to haemoconcentration with 'sludging' in diabetic patients with significant peripheral arterial disease) and recent studies have been more reassuring.23 In Yuan et al’s real-world study, published this year, no evidence was found for an increased risk of below knee lower extremity amputation for new users of canagliflozin compared with non-SGLT2 inhibitor glucose lowering drugs in patients with T2D.23 Overall, then, the risk:benefit ratio should be weighed up for each individual patient. If someone has evidence of peripheral arterial disease, this suggests that they are an arteriopath with an increased risk of other manifestations of CVD. As indicated by the EMPA-REG and CANVAS studies, these are precisely the sort of patients with most to gain from an SGLT2 inhibitor. Pragmatically, meticulous foot care should be practised by all people living with diabetes and those who care for them in order to minimise the risk of LLA.
BIOETHICAL PRINCIPLES
Bioethical principles should underpin the care we offer to patients, no matter what they are attending for. Bioethical principles include the concepts of autonomy, beneficence, non-maleficence and justice.24 Autonomous decision making should be encouraged but this can only be truly implemented if patients are aware of the risks and benefits of any intervention and similarly only competent, knowledgeable health care professionals can offer the necessary information to enable people to be truly autonomous. It is important to take time to learn about the subject areas you practise in and also to offer opportunities for discussion for people who are deciding about the best way to manage their condition and minimise the risk of complications.
CONCLUSION
The management of T2D combines lifestyle interventions and pharmacological therapies. The cardiovascular complications of diabetes, both macrovascular and microvascular, cause significant morbidity and mortality and most of the money the NHS spends on diabetes is spent on treating these complications, rather than the condition itself. When introducing or intensifying drug treatment in diabetes, consideration should be given to potential risks and benefits. Metformin, SGLT2 inhibitors and one GLP1, liraglutide, all have evidence of cardiovascular benefits. The SGLT2 inhibitor canagliflozin has also shown evidence of benefit in patients with CKD.8 These benefits contrast sharply with drugs where there is evidence of increased harm, such as sulfonylureas,22 or evidence of an impact on heart failure such as pioglitazone, saxagliptin and alogliptin.20,21
Studies into the risks and benefits of these and other glucose lowering drugs are continuing and clinicians should keep abreast of developments. This will ensure that they can promote professionalism and trust, through their ability to promote autonomous decision making by patients who may have much to gain from therapies which have evidence of benefit beyond improved glycaemic control. Differences may occur even within class so that evidence for one treatment may be stronger than another. Local guidelines are not always up to date with latest evidence and may also reflect a financial position rather than the clinically best option. General practice nurses should be aware of the licensed indications for any drugs that they may recommend and/or prescribe and recognise that these can change when new evidence becomes available in this fast changing subject area.
Napp Pharmaceuticals Ltd has sponsored production of this article but has had no editorial input or influence over the final content. Napp Pharmaceuticals Ltd has reviewed the article for factual accuracy only
UK/DIA-18074
REFERENCES
1. Leon BM, Maddox TM. Diabetes and cardiovascular disease: epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes 2015;6(13):1246-58
2. Fowler MJ. Microvascular and Macrovascular Complications of Diabetes. Clin Diabetes 2008;26(2):77-82
3. Haffner SM, Lehto S, Rönnemaa T, et al. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339:229–34
4. Narres M, Claessen H, Droste S, et al. The Incidence of End-Stage Renal Disease in the Diabetic (Compared to the Non-Diabetic) Population: A Systematic Review. PLoS ONE 2016;11(1): e0147329. https://doi.org/10.1371/journal.pone.0147329
5. Diabetes UK (2014) The Cost of Diabetes Report https://www.diabetes.org.uk/resources-s3/2017-11/diabetes%20uk%20cost%20of%20diabetes%20report.pdf
6. Scottish Intercollegiate Guidelines Network. SIGN 154 Pharmacological management of glycaemic control in people with type 2 diabetes, 2017 http://www.sign.ac.uk/assets/sign154.pdf
7. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes N Engl J Med 2015;373:2117-2128 DOI: 10.1056/NEJMoa1504720
8. Neal B, Perkovic V, Mahaffey KW, et al, on behalf of the CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med 2017;377:644-57
9. Wiviott SD, Raz I, Bonaca MP, et al. The design and rationale for the Dapagliflozin Effect on Cardiovascular Events (DECLARE)–TIMI 58 Trial. Am Heart J 2018;200:83-89
10. AstraZeneca. Press release, 24 September 2018. https://www.astrazeneca.com/media-centre/press-releases/2018/farxiga-achieved-a-positive-result-in-the-phase-iii-declare-timi-58-trial-a-large-cardiovascular-outcomes-trial-in-17000-patients-with-type-2-diabetes-24092018.html
11. Wanner C. EMPA-REG OUTCOME: the nephrologist's point of view Am J Med 2017;130:S63-S72
12. Mazidi M, Rezaie P, Gao HK, Kengne AP. Effect of sodium-glucose cotransport-2 inhibitors on blood pressure in people with type 2 diabetes mellitus: A systematic review and meta-analysis of 43 randomized cohort trials with 22 528 patients. J Am Heart Assoc 2017:6:e004007. doi:10.1161/JAHA.116.004007
13. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016; 375:311-322 DOI: 10.1056/NEJMoa1603827
14. Holman RR, Bethel MA, Mentz RJ, et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes N Engl J Med 2017;377:1228-1239 DOI: 10.1056/NEJMoa1612917
15. Tucker ME. Canagliflozin Renal Outcomes Study Is Halted Early for Efficacy. Medscape 2018 https://www.medscape.com/viewarticle/899424
16. De Cosmo S, Viazzi F, Pacilli A, et al. Predictors of chronic kidney disease in type 2 diabetes: A longitudinal study from the AMD Annals initiative. Medicine (Baltimore) 2016;95(27):e4007
17. Boehringer Ingelheim. Empagliflozin (Jardiance®) to be studied in chronic kidney disease. Press release, 12 June 2017. https://www.boehringer-ingelheim.com/press-release/empagliflozin-be-studied-chronic-kidney-disease
18. Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am. J. Cardiol 1974;34(1):29–34.
19. Dei Cas A., Khan S.S., Butler J., et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail 2015;3(2):136–145.
20. Actos (pioglitazone). Summary of Product Characteristics. Takeda UK Ltd. Electronic Medicines Compendium, 2016 https://www.medicines.org.uk/emc/product/1287/smpc
21. FDA Drug Safety Communication: FDA adds warnings about heart failure risk to labels of type 2 diabetes medicines containing saxagliptin and alogliptin, 2018 https://www.fda.gov/Drugs/DrugSafety/ucm486096.htm
22. European Medicines Agency. SGLT2 inhibitors: information on potential risk of toe amputation to be included in prescribing information, 2017.
23. Yuan Z, DeFalco FJ, Ryan PB, et al. Risk of lower extremity amputations in people with type 2 diabetes mellitus treated with sodium?glucose co?transporter?2 inhibitors in the USA: A retrospective cohort study. Diabetes Obes Metab 2018;20(3):582–589. doi: 10.1111/dom.13115
24. Beauchamp TL and Childress JF. Principles of biomedical ethics. New York: Oxford University Press; 2013
25. Krepinsky J, Ingram AJ, Clase CM. Prolonged sulfonylurea-induced hypoglycemia in diabetic patients with end-stage renal disease Am J Kidney Dis 2000;35(3):500-505