Transforming diagnosis: identifying and breaking down barriers to early diagnosis of ovarian cancer
Catherine Pearson
Catherine Pearson
Interim Clinical Change Manager
Amy Schofield
Senior Healthcare Engagement Officer,
Target Ovarian Cancer
Practice Nurse 2023;53(3):15-19
An award-winning project from Target Ovarian Cancer has demonstrated that three simple primary care interventions can make a difference in ovarian cancer diagnosis. Here’s how you can implement these changes in your practice to transform the future of ovarian cancer care at a local level.
Eleven women die every day from ovarian cancer because diagnosis is often too late.1 Research from Target Ovarian Cancer has highlighted the urgent need for ovarian cancer to be recognised as a significant national priority, and for action in improving diagnosis, treatment and outcomes.2 Early diagnosis saves lives, and GPs and primary care teams play a hugely important role in helping women with symptoms access diagnostic tests quickly.
We know that faster and earlier diagnosis saves lives – the quicker the diagnosis is received, the more quickly the woman can be set on the right treatment pathway.
WHY EARLY DIAGNOSIS MATTERS
Two thirds of cases are diagnosed too late, when the cancer is harder to treat.3 The statistics are stark:
- Stage 1: almost 95% survive for 5 years4
- Stage 4: almost 15% survive for 5 years
- 50% of women are diagnosed at stage 3 and 45
Sadly, we know that one in seven women (14%) die within two months of an ovarian cancer diagnosis.5
The earlier and faster ovarian cancer is diagnosed, the greater the chance of receiving treatment and the greater the chance of survival.
REGIONAL VARIATION
At Target Ovarian Cancer, we know that there’s an unacceptable variation in the diagnosis of ovarian cancer happening across the country. This urgently needs to change.
Target Ovarian Cancer developed and tested three decision-making tools in collaboration with regional partners to see if progress can be made. We found that it can. (See Variation in diagnosis of ovarian cancer ‘unacceptable’. Practice Nurse 2023;53(2): online only.
We know that there are challenges facing primary care in setting women on the right treatment pathway. The primary symptoms can be confused with other conditions, such as irritable bowel syndrome (IBS), diverticulitis and recurrent urinary tract infections (UTIs). Public awareness remains low, which means that early symptom presentation from patients remains a significant and ongoing concern for primary care. However, positive change is possible.
This is why the Transforming diagnosis: identifying and breaking down barriers to early diagnosis6 project came about. This innovative project could transform the rate of early diagnosis of ovarian cancer in primary care and here’s how it could be implemented in your practice.
Primary care plays a vital role in getting the right diagnosis of ovarian cancer, and as practice nurses and advanced nurse practitioners you are well positioned to spot the signs and symptoms of ovarian cancer in the women that you see every day. The outcomes for women diagnosed via an emergency presentation at A&E are much poorer than those diagnosed through primary care.5 Target Ovarian Cancer’s Pathfinder 2022 report2 demonstrates that there are still too many delays along the diagnostic pathway and that primary care clinicians want more training and support to help them to ensure that no-one slips through the net.
Target Ovarian Cancer has been working in partnership with Cancer Alliances and Primary Care Networks to develop and test interventions to help speed up diagnosis. Our interventions have been welcomed by primary care networks and healthcare professionals, and show promise in helping to minimise the risk of misdiagnosis.
Results from the pilots have now been published, alongside:
- An Early Diagnosis toolkit – Protocols and templates for EMIS Web
- A new Target Ovarian Cancer Early Diagnosis Network to bring together all health care professionals with an interest in improving diagnosis of ovarian cancer in the UK. Sign up at https://targetovariancancer.org.uk/health-professionals/early-diagnosis-network.
THE INTERVENTIONS
We designed and tested three digital interventions to address late diagnosis in this ground-breaking project.
We worked collaboratively with primary care clinicians, data managers and cancer project leads in different regions to deliver these digital interventions in primary care:
- A clinical IT alert tool
- A retrospective audit search
- A safety netting search
The regional collaborations found that the focused interventions worked effectively to minimise late and/or misdiagnosis and were easy to implement and incorporate into routine practice.
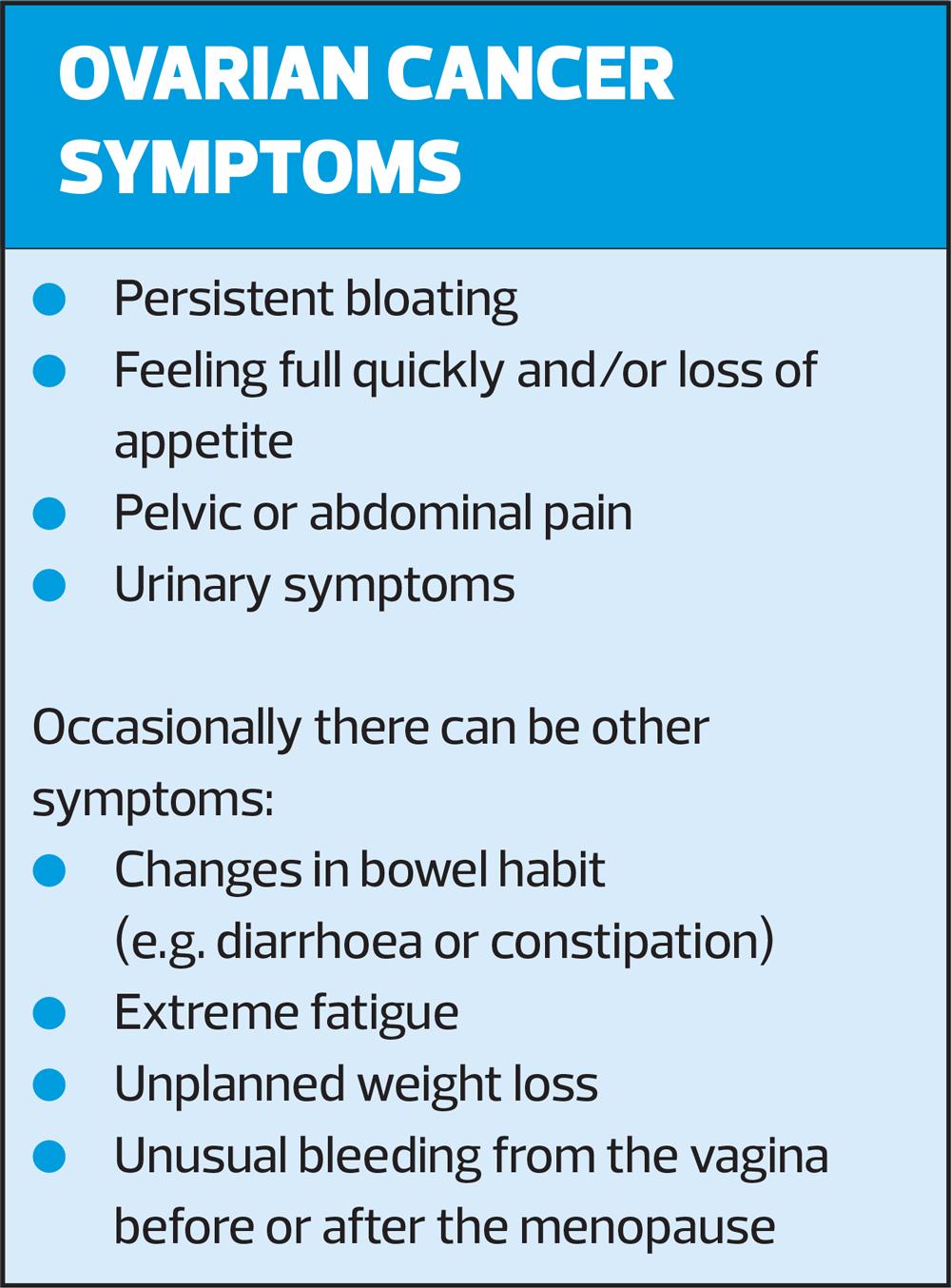
The symptoms of ovarian cancer can include persistent bloating, abdominal pain and loss of appetite, problems which can also present in benign disease such as IBS. This means that some patients with these symptoms are not immediately investigated for ovarian cancer.
By working together with primary care in three regions in England, our research has shown that these interventions can be implemented easily,7 and help clinicians in primary care to:
- Consider and act confidently on possible ovarian cancer symptoms
- Recall women with possible ovarian cancer symptoms who have not had a CA125 test
- Safety net women who have persistent symptoms but whose CA125 and ultrasound scan are reported as normal.
These are important, lifesaving actions that will reduce misdiagnosis and speed up referral of unwell patients to the right pathway for them. They can be implemented cheaply and simply and can become routine in any practice – across the primary care team – to support earlier diagnosis of ovarian cancer.
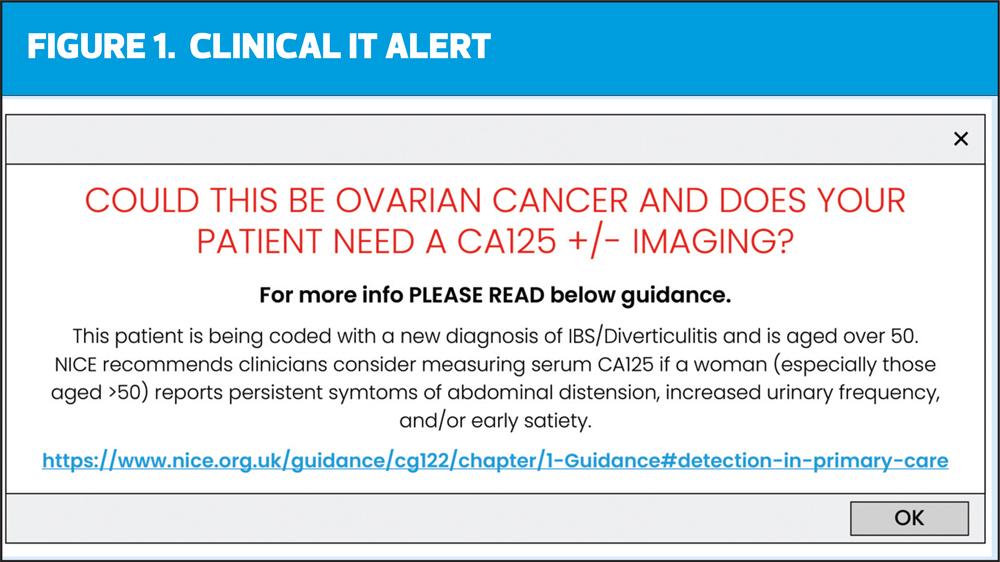
Clinical IT Alert
To support GPs to consider ovarian cancer, we tested an IT alert that comes up on screen (with advice to test CA125 and review NICE guidance) when a woman over 50 is coded with a new diagnosis of IBS or diverticulitis and there has been no recent CA125 (Figure 1).
A clinical IT alert protocol for EMIS Web was developed and tested by four PCNs in Pennine Lancashire between December 2021 and May 2022.
All staff participating in the evaluation agreed that the clinical IT alert helped them to consider ovarian cancer as a possible diagnosis. They also agreed that the alert was simple to upload and use and that they wanted to keep it on their system.
Retrospective audit search
This intervention is an audit search that brings up a list of women coded with a new diagnosis of IBS or diverticulitis in the last six months, with no recent CA125 result. This search provides an opportunity for the clinical team to review if further action is needed and invite patients back for further investigation if appropriate.
More than 90% of participants in the evaluation agreed that the audit helped them to identify possible misdiagnosis of ovarian cancer.7 Feedback included that the audit created a beneficial learning exercise for all staff within primary care and improved their knowledge of ovarian cancer.
Safety netting search
This is a safety netting search that brings up a list of women with a recent normal CA125 blood test result, so clinical staff can review them for follow up and potential further testing if symptoms have persisted.
This search was carried out by four PCNs in Pennine Lancashire, identifying 402 women. Of these, 365 were contacted and given advice about persistent symptoms and returning to their GP. All clinical staff found the normal CA125 monitoring a worthwhile exercise for them and their patients. They also agreed that this helped them to provide an effective safety netting system for their patients. The workload was generally reported as positive and manageable.
In summary
- All three digital based interventions were evaluated by primary care teams as effective support tools to diagnose patients who might otherwise be missed.
- Use of the tools allowed clinicians to identify two patients in Pennine Lancashire who had been misdiagnosed and improve their care.
- The clinical IT alert received the most positive feedback of the three clinical patient management tools in Pennine Lancashire.
Our evaluation concludes that incorporating clinical IT alerts and patient data searches into primary care to facilitate earlier diagnosis of ovarian cancer, amongst other things, requires ease of use of the tools; assigning audit and safety netting tasks to a specific clinician, such as Physician Associates; a consistent approach to coding symptoms and diagnoses across clinical and administrative teams; and education for primary care teams on the value of CA125 blood tests for managing and safety netting patients with symptoms of ovarian cancer.
The pilots and interventions have helped to increase clinical awareness, investigation and management of symptomatic ovarian cancer presentation, underpinning and reinforcing good practice as recommended by NICE guidance.8
OPPORTUNISTIC CONVERSATIONS
Target Ovarian Cancer’s Pathfinder research found that 40% of women wrongly believe that cervical screening detects ovarian cancer, and the report recommended that the information provided at cervical screening appointments ‘must make it clear that it does not test or screen for other gynaecological cancers’.2 Women will often speak to nurses more during these routine women’s health checks. This presents an opportunity for practice nurses to potentially intervene in an opportunistic way.
Please use cervical screening appointments to share with your patients that ovarian cancer cannot be detected by a cervical screening test, tell them the symptoms to look out for, and advise that if they have any of the symptoms of ovarian cancer, they should make an urgent appointment with their GP. Please also ask younger women to tell their mothers, aunts, friends about this, and the symptoms to look out for, spreading the word as far as possible.
Urine diptests
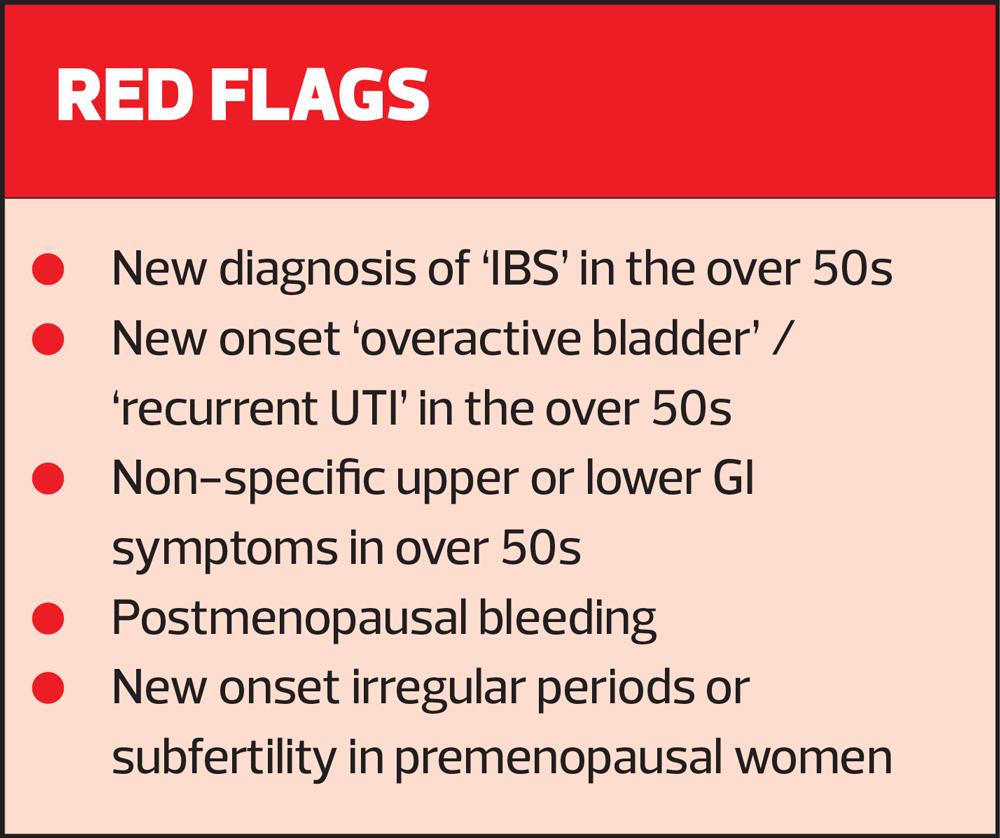
If you are doing a urine test on a woman and it is negative, then take this opportunity to talk to the patient about possible causes of urinary symptoms such as menopause, bladder problems and ovarian cancer. Repeat clear mid-stream urine results should be considered with caution, particularly if the patient is >50, as this can be a red flag for ovarian cancer.
Encourage your patient to keep a symptoms diary, so that any patterns/persistence are highlighted. You can download our symptoms diary at https://targetovariancancer.org.uk/sites/default/files/2021-01/Target%20Ovarian%20Cancer%20symptoms%20diary.pdf.
However, patients should still book an appointment with their GP and not delay this for the purpose of keeping a symptoms diary.
In addition to looking out for the symptoms of ovarian cancer, if your patients mention that the symptoms are…
- New – they're not normal for the patient
- Frequent – they usually happen more than 12 times a month
- Persistent – they don't go away
…consider ordering a CA125 test.
NICE recommends:
- Measuring serum CA125 in primary care in women with symptoms that suggest ovarian cancer.
- If serum CA125 is 35 IU/ml or greater, arranging an ultrasound scan of the abdomen and pelvis.8
For any woman who has normal serum CA125 (less than 35 IU/ml), or CA125 of 35 IU/ml or greater but a normal ultrasound, NICE recommends:
- Assessing her carefully for other clinical causes of her symptoms and investigate if appropriate
- If no other clinical cause is apparent, advise her to return to her GP if her symptoms become more frequent and/or persistent.8
WHAT IS THE CA125 TEST?
Cancer Antigen 125 (CA125) is a protein that is produced from foetal coelomic epithelium. This means the mullerian structure (tubes, uterus, cervix etc), pericardium, peritoneum.
Anything that stretches the peritoneum or irritates the above structures can cause a rise in CA125.
A normal level of CA125 is usually less than 35 units per millilitre (IU/ml), however some women do have a naturally high level of CA125 in their blood. The level of CA125 can rise for many reasons, not only in ovarian cancer.
Most women with a result below 35 IU/ml won't have ovarian cancer. But a small number of women with ovarian cancer will have a CA125 test result below 35 IU/ml. The key is to listen to the patient and if they return with continuing and/or worsening symptoms then a further CA125 test should be recommended within four to six weeks.
Differential diagnosis for raised CA125
In premenopausal women:
- Menstruation
- Ovulation
- Endometriosis
- Fibroid
- PID
In elderly women with comorbidities:
- Cardiac failure
- Renal failure
- Hepatic failure
- Other cancer
- Any other reason that can cause irritation of the peritoneum
If a woman has a normal CA125 but is symptomatic, ask them to return if those symptoms persist/get worse, and consider a repeat CA125 in four to six weeks.
- Over 80% of women with advanced ovarian cancer will have a raised CA125
- Certain types do not raise CA125
- 50% of women with stage 1 ovarian cancer will have a normal CA125
- There is no role for screening of women with no family history of ovarian cancer.
Please signpost your patients undergoing diagnostic tests to our nurse-led support line for advice, information and support on 020 7923 5475.
REFERENCES
1. Cancer Research UK. Ovarian cancer by mortality; 2020 Available at: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/ovarian-cancer/mortality#heading-Zero
2. Target Ovarian Cancer. Pathfinder 2022: Faster, further, and fairer. Available at: https://targetovariancancer.org.uk/get-involved/campaign/policy/pathfinder
3. National Cancer Registration and Analysis Service. Stage breakdown by CCG 2017; 2019. http://www.ncin.org.uk/publications/survival_by_stage
4. Cancer Research UK. Ovarian cancer survival; 2021 https://www.cancerresearchuk.org/about-cancer/ovarian-cancer/survival
5. The Ovarian Cancer Audit Feasibility Pilot :Outputs; 2020. https://targetovariancancer.org.uk/get-involved/campaign/policy/ovarian-cancer-audit-feasibility-pilot and https://digital.nhs.uk/data-and-information/publications/statistical/ovarian-cancer-audit-feasibility-pilot
6. Target Ovarian Cancer (2023) Identifying and breaking down barriers to early diagnosis of ovarian cancer in primary care: Interventions and learnings; 2023 https://targetovariancancer.org.uk/breaking-down-barriers-early-diagnosis-ovarian-cancer
7. World Ovarian Cancer Coalition Impact Awards. Most Inspiring Collaboration Award; 2022 https://targetovariancancer.org.uk/news/target-ovarian-cancer-win-most-inspiring-collaborations-award
8. NICE CG122. Ovarian cancer: recognition and initial management of ovarian cancer; 2011 https://www.nice.org.uk/guidance/cg122

Related articles
View all Articles