|
January 2020 Asthma reviews: a new look Asthma reviews are an opportunity to assess control, identify modifiable risk factors for poor outcomes and optimise management appropriately – particularly after asthma attacks, which are a signal that further action is neededAsthma reviews are an opportunity to assess the effect the disease is having on someone’s life, to identify how well the asthma is controlled and to optimise management. As asthma is a complex, potentially fatal disease, these reviews must, in my view, be conducted by people trained and competent to do so, with frequent updates and peer review. Sadly, particularly in the UK, this role has often been inappropriately delegated to untrained individuals, sometimes with fatal consequences.1 Asthma reviews should be conducted routinely, but since symptoms and airflow obstruction fluctuate from time to time, it is illogical to simply rely on an annual check-up of the patient’s ‘current status’ using a test like the Asthma Control Test (ACT) or the unvalidated Royal College of Physicians 3 Questions (RCP-3Qs). An asthma attack (flare-up or exacerbation) is a clear signal that something serious has gone wrong and urgent action is required. Therefore, in addition to ‘routine’ reviews, this article will discuss opportunistic asthma reviews, particularly following attacks and changes in medication. While there are two UK asthma guidelines,2,3 I have referred extensively to the Global Initiative for Asthma (GINA) strategy documents.4 I am on the board of the latter, and while there are some strengths in the UK guidelines, I believe the guidance provided by GINA is more practical for non-academic generalists in primary and secondary care. Furthermore, GINA is the only guideline that is updated annually, based on all the evidence published during the preceding year. COMPONENTS OF AN ASTHMA REVIEW Asthma reviews, whether routine or opportunistic, should include the following:
Both opportunistic asthma reviews (when patients consult for something else) and those planned to evaluate the effect of a change of inhaler device or medication, usually 6-12 weeks after the change, should focus on assessing current control and identifying risk. In addition to identifying modifiable risk, post attack reviews performed within a few days of treatment for the attack should include identification of ‘red flag’ signs and assessment of current control to determine whether the attack is resolving or over. If not, the clinician should take immediate action to optimise care to resolve the attack. ASTHMA DIAGNOSISAsthma is ‘… a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath and cough that vary over time and in intensity, together with variable expiratory airflow limitation.’4 During any asthma review, particularly where there is evidence of poor control, it is essential that the diagnosis is confirmed. Check for:
If lung function hasn’t been recorded, this should be done, either with PEF or quality assured spirometry and reversibility, or a home PEF diary chart with subsequent review. If there is sufficient evidence confirming the diagnosis, this should be entered with the relevant computer code. If not, but asthma is still suspected, then a code for suspected asthma should be entered. There are a number of different phenotypes and endotypes of asthma and further clues supporting the diagnosis include biomarkers such as raised eosinophils or a raised Fractional exhaled Nitric Oxide (FeNO) in patients with Type-2 inflammation asthma. (Box 1) However, bear in mind that these features may not be present and their absence does NOT exclude the diagnosis.4 Other endotypes, such as non-eosinophilic or paucigranulocytic asthma may be present. Therefore, if the diagnosis cannot be established, consider referring patients who remain poorly controlled despite treatment to specialists for evaluation. ASTHMA CONTROLSymptom controlIn the UK, largely as a result of the demands of the Quality Outcome Framework (QOF), current symptom control is assessed exclusively using the RCP-3Qs. This is an unvalidated test and is not applicable in children under 16 years of age. The more robust Asthma Control Test (ACT) (https://www.asthmacontroltest.com/Europe/United%20Kingdom/en) is validated, is used by a number of clinicians and in many research studies.2 The ACT (or cACT for children under 11) has a major advantage in that a score is generated: ≥ 19 represents good symptom control, 16-19 is not well controlled, and ≤ 15 is very poorly controlled. This test is useful for assessing patients’ progress, for example after initiating treatment or after a change in treatment, and the minimally important clinical difference, when interpreting change, is 3 points. This is very useful in assessing response to changed therapy after 6–12 weeks. However, it is important to note these assessments only establish how the person’s asthma is currently controlled, and at most for the previous month or so. As the disease can flare up at any time, it is clearly illogical to simply assess current symptoms in people with asthma. Future riskFuture risk is an additional domain assessed when determining a patient’s asthma control.4 Failure to identify risk was highlighted in the UK National Review of Asthma Deaths (NRAD) in 2014,1 and the concept has been included in the 2019 update of the British Thoracic society (BTS)/Scottish Intercollegiate Guideline Network (SIGN) UK asthma guidelines.2 (Table 1) Asthma control is important in defining three phenotypes of asthma: uncontrolled, difficult to treat and severe asthma. (Box 2) In practice, by using both of these domains (symptoms and risk) for assessing asthma control, clinicians are more able to identify those patients in need of optimisation of care or referral to a specialist. Table 1 from GINA combines an assessment of symptom control and also of future risk. While someone with symptoms is clearly at risk, from the table it is evident that even if someone does not have current symptoms or is requiring as-needed reliever therapy, they may still be at risk. The latest BTS/SIGN guideline tables 9 and 10 also include future risk in adults and children.2 The guideline grades the relative risk of these factors. In my view, while there is possible academic value in ascribing relative risk, there is little clinical advantage in stating that one risk is less important than another. My recommendation would be to treat patients who have any risk factors for poor outcome with great care, and, if appropriate, with advice from a respiratory specialist. ASTHMA SEVERITYAsthma severity is defined retrospectively, based on the combination of drug treatment and level of control.5 Severity of asthma is not the same as the level of treatment prescribed. For example, one cannot assume that a patient has mild asthma based on the fact they have only been prescribed a reliever inhaler. Simply put, a patient who continues to suffer from asthma attacks or symptoms despite correctly taking high dose drug treatment is defined as having ‘severe asthma’. This is one of the reasons why I state that a single annual asthma review based on current symptoms is illogical. A common misconception is that people with mild asthma are not at risk, the main problem being that severity is not often assessed using the above definition of the 2014 task force.5 Around six out of ten (58%) of those who died from asthma in the NRAD report were classified as having ‘mild’ or ‘moderate’ asthma.1 Furthermore, there are a number of studies demonstrating that patients perceived to have mild asthma, and only prescribed as-needed relievers, are at risk of attacks. In one example where patients were prescribed salbutamol only, 23.3% had required urgent healthcare for asthma in the previous year.6 In another study, where investigators assessed over 90 studies reporting on patients with apparent mild asthma, having symptoms weekly or less in the previous three months, 30–37% had acute asthma attacks, 16% had near fatal asthma and 15–20% died from acute asthma.7 These studies highlight that all patients with asthma are potentially at risk. Therefore health care professionals caring for people with asthma must be appropriately trained to do so. About 20% of patients have difficult to treat asthma, i.e. they remain symptomatic despite prescriptions for high dose drug treatment. The majority of these patients can be controlled by ensuring adequate preventer treatment is prescribed, collected and taken, using correct inhaler technique. It is important to identify and record the severity of a patient’s asthma because those with severe asthma must be referred to someone with expertise in that area, both to confirm the diagnosis and also to evaluate suitability for biologic treatments. Sadly, a recent study showed that less than 25% of adults with severe asthma were referred to specialists.8 ADHERENCEHealth professional adherence to guidelines and guidance can help to ensure patient safety; therefore it is incumbent upon those delegating care, as well as the providers of it, to ensure that anyone caring for people with asthma is appropriately trained and competent. This includes those responsible for prescribing, or performing asthma reviews as well as management of asthma attacks. Poor patient adherence to medical advice, including failure to collect, take or administer medication and failure to attend for reviews, increases the risk of poor asthma outcomes, including attacks and deaths. Control of asthma for many patients with difficult to treat asthma can be improved significantly through improving adherence, usually through explaining the way the medication works and the possible risks associated with inadequate medication. INHALER TECHNIQUEMuch emphasis is placed on the cost of prescribed medication and much pressure applied to clinicians to reduce waste and keep costs as low as possible. In the case of drugs delivered by an inhaler device the greatest waste is incurred when these are prescribed without teaching and ensuring patients can use the devices correctly. The most expensive inhaler is the one the patient can’t (or won’t) use! Incorrect device technique is associated with poor asthma control, increased attacks and hospitalisations,9 and this has not improved over the last 40 years.10 This is further complicated by the increasing numbers of different devices available, and the fact that most health professionals cannot use the devices correctly themselves.11 Furthermore, there is evidence that patient preference for a device can improve outcome, so in addition to ensuring patients can use the device, clinicians should also ensure they are satisfied with it.12 PATIENT EDUCATIONAmong the deaths investigated in the NRAD report, 45% occurred in people who did not either call for or get medical help during their final, fatal attack.1 This is unsurprising, because 77% of those who died had no recorded evidence that they had been issued with a personal asthma self-management action plan explaining how and when to get medical assistance. Plans can range from very simple advice, like ‘see me urgently if you start wheezing or coughing’, to a detailed set of instructions. The key is to tailor the advice and plan to the age, aptitude and ability of the patient, and to update it whenever medication is changed, or post attack if appropriate. Available plans include the adult and child ones produced by Asthma UK, the example on the GINA website and the one on my own website. (See Resources) In my view, plans should include written instructions for patients to ensure they consult their asthma health care professional within a few days after treatment for an attack. OPTIMISING DRUG TREATMENTClearly, if a person’s asthma is uncontrolled, their medication should be reviewed and optimised. Guideline documents include fairly detailed advice on medication and dosages and these usually follow a stepwise pattern of advice, where this is increased or decreased depending on the patient’s level of control. An assessment of appropriateness of prescriptions and adherence should be included in any asthma review, and the reader is advised to be familiar with the latest guidance for their locality. Furthermore, it is important to be aware that excess reliance on short acting bronchodilator reliever medication and insufficient preventer medication are both independent risk factors of poor asthma outcome, including symptoms, attacks and death.1,2,4 POST ATTACK REVIEWAsthma attacks are episodes occurring in people with asthma where their symptoms have flared up and which may be associated with fluctuation of lung function and oxygen saturation. Attacks vary in severity from mild to life threatening events and attack severity is determined on the basis of a detailed clinical assessment of lung function, oximetry, vital signs and response to treatment. (see SIGN/BTS 158, Tables 15 and 17 at https://www.sign.ac.uk/assets/sign158.pdf).2 No-one knows how long an asthma attack will last, yet in most cases, irrespective of the severity of asthma, oral corticosteroid courses limited to three or five days are prescribed, often without any advice or arrangements for follow up. The UK guidelines have stated clearly, since 1996, that attacks should be treated with oral corticosteroids until the attack has resolved.2 This is why it is so important to ensure patients have a post attack review before they run out of their oral corticosteroids. (Figure 1) A post attack review has two purposes (see Figure 1): firstly to determine whether the attack is resolving. This is determined on the basis of the presence of any ‘red flag signs’ such as:
If the attack has worsened or is not resolving, either the course of oral corticosteroids should be extended, or the patient should be sent to hospital urgently, depending on the findings. Clearly the patient should be reviewed as needed until the attack has resolved. Two possible major challenges are the current UK practice of paediatric prescribing of high dose salbutamol ‘weaning plans’ (10 puffs 4 hourly), which is unlicensed and for which there is no evidence, and the emerging practice of prescribing a single dose of dexamethasone pre-discharge for children treated in hospital for asthma attacks. The first is potentially dangerous, because it can induce bronchospasm and removes the danger sign for parents related to poor response to relievers.13 The second is an unwise, and as yet relatively untested treatment for acute attacks, mainly because those of us working in the community will be doing the follow up reviews without being clear on the status of the dexamethasone prescribed, and whether it would be safe to extend the course without knowing what the steroid blood levels are. The second reason for performing a post-attack review is to assess the patient’s risk status and then to act on the presence of any modifiable risk factors for poor outcomes discussed in the section above on asthma control.(See Table 1) CONCLUSIONThis article summarises a personal view on performing asthma reviews in primary care. These should always be done by appropriately trained individuals and with the overall aims of:
In the UK, asthma is still responsible for unacceptably high levels of preventable morbidity and mortality in comparison with other countries. If we are to make an impact we need to move away from a ‘tick box’ exercise to more appropriate routine and opportunistic reviews that properly assess asthma control and future risk. REFERENCES1. Why asthma still kills: the National Review of Asthma Deaths (NRAD) Confidential Enquiry report: Royal College of Physicians. London; 2014 https://www.rcplondon.ac.uk/sites/default/files/why-asthma-still-kills-full-report.pdf. 2. Scottish Intercollegiate Guideline Network (SIGN), the British Thoracic society (BTS). British guideline on the management of asthma; 2019 https://www.sign.ac.uk/sign-158-british-guideline-on-the-management-of-asthma.html. 3. NICE NG80. Asthma: diagnosis, monitoring and chronic asthma management; 2017 https://www.nice.org.uk/guidance/ng80 4. The Global Strategy for Asthma Management and Prevention, Global Initiative for Asthma (GINA); 2019. https://www.ginasthma.org. 5. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 2014;43:343-73. 6. Reddel HK, Ampon RD, Sawyer SM, Peters MJ. Risks associated with managing asthma without a preventer: urgent healthcare, poor asthma control and over-the-counter reliever use in a cross-sectional population survey. BMJ Open. 2017;7. 7. Dusser D, Montani D, Chanez P, et al. Mild asthma: an expert review on epidemiology, clinical characteristics and treatment recommendations. Allergy. 2007;62(6):591-604. 8. Bloom CI, Walker S, Quint JK. Inadequate specialist care referrals for high-risk asthma patients in the UK: an adult population-based cohort 2006–2017. J Asthma. 2019:1-7. 9. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respiratory Medicine 2011;105(6):930-8. 10. Sanchis J, Gich I, Pedersen S. Systematic Review of Errors in Inhaler Use: Has Patient Technique Improved Over Time? Chest 2016;150(2):394-406. 11. Plaza V, Giner J, Rodrigo GJ, Dolovich MB, Sanchis J. Errors in the Use of Inhalers by Health Care Professionals: A Systematic Review. J Allergy Clin Immunol Pract. 2018;6(3):987-95. 12. Plaza V, Giner J, Calle M, et al. Impact of patient satisfaction with his or her inhaler on adherence and asthma control. Allergy Asthma Proc. 2018;39(6):437-44. 13. Levy ML, Fleming L, Warner JO, Bush A. Paediatric asthma care in the UK: fragmented and fatally fallible. Br J Gen Pract 2019;69:405-6. |
Dr Mark L Levy FRCGP Locum general practitioner; Clinical lead National Review of Asthma Deaths (NRAD) 2011-2014; Board member Global initiative on Asthma (GINA)  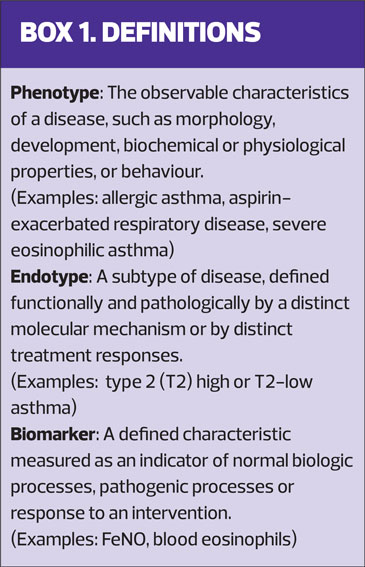 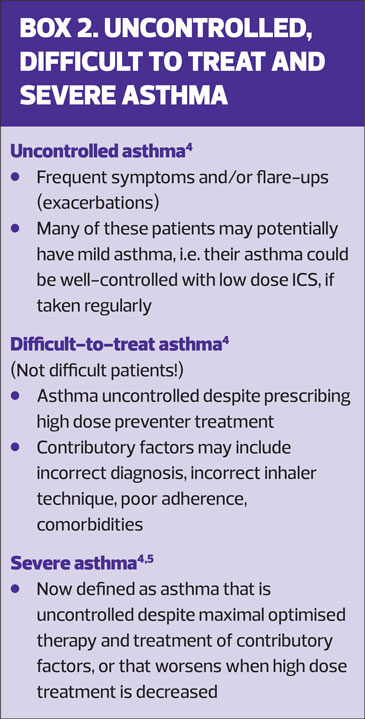 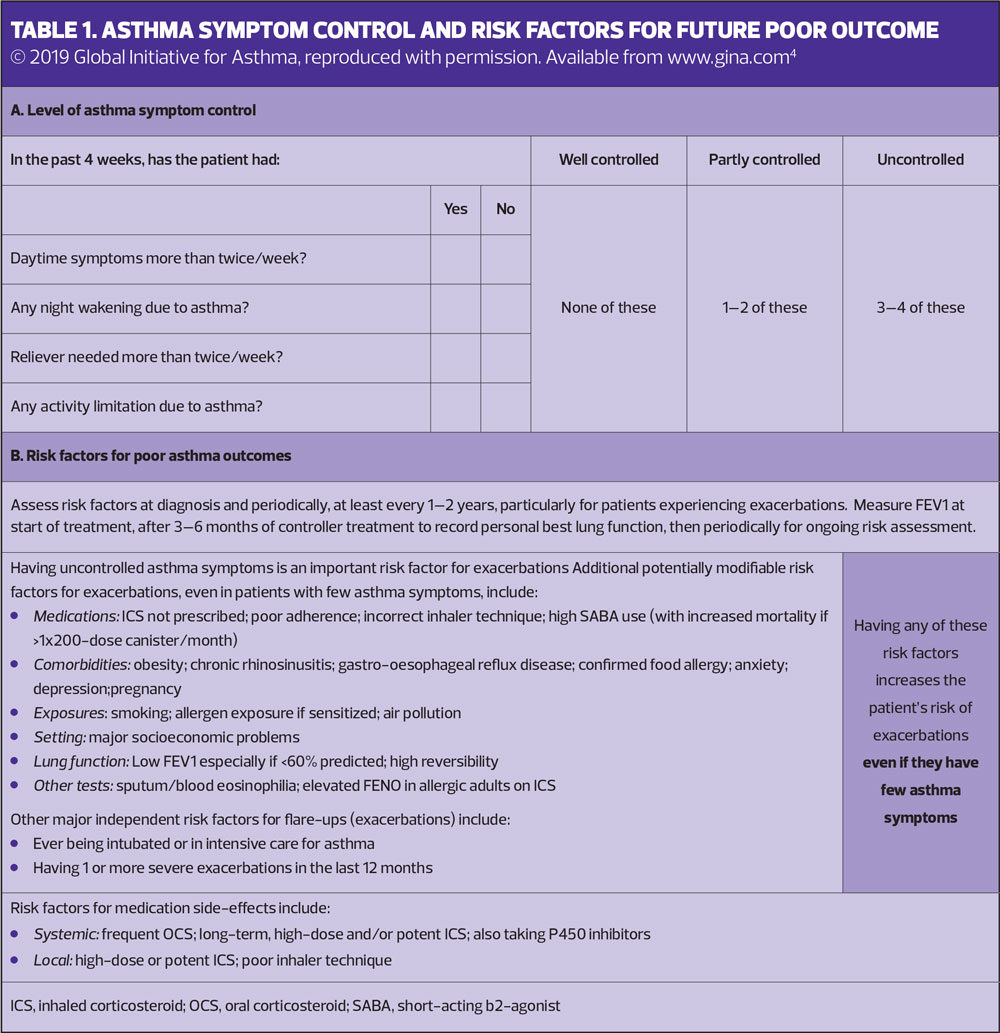 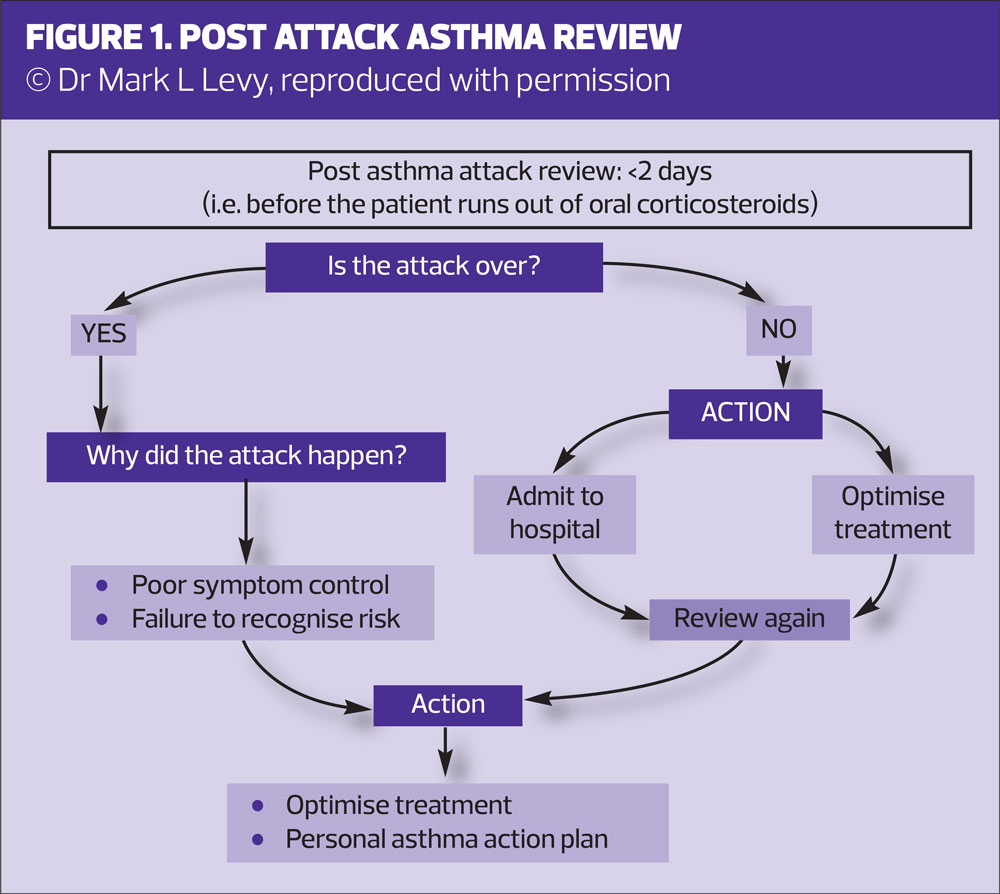        |
Back to top